
Case
A 58 year old man presented with intermittent chest pain for 2 weeks. He has active pain at the time of this initial ECG:
Analysis
To me this is clearly an anterior STEMI, and it meets STEMI criteria even for someone under age 40 (at least 2.5 mm in V2 and V3, as measured at the J-point, relative to the PQ junction).
On the other hand, normal variant ST Elevation (often called early repolarization) may also have very marked ST elevation. So when there is upward concavity in all of V5-V6, absence of any ST depression, and absence of Q-waves, it still might be early repol and the computer might not call this anterior STEMI. Even the most contemporary algorithms are very inaccurate (see references below).
Thus, it is useful to use the STEMI-early repol calculator
(which is not, as far as I know, programmed into automated interpretation algorithms):
You can find the calculator here:
--- (http://hqmeded-ecg.blogspot.com/p/rules-equations.html)
--- Or use the free iPhone app ("subtleSTEMI): https://itunes.apple.com/us/app/subtlestemi/id617146818?mt=8
---Or go to www.mdcalc.com: https://www.mdcalc.com/subtle-anterior-stemi-calculator
The QTc = 455
ST Elevation at 60 ms after the J-point (STE60V3) = 4mm
R-wave amplitude in V4 (RAV4) = 17 mm
A 58 year old man presented with intermittent chest pain for 2 weeks. He has active pain at the time of this initial ECG:
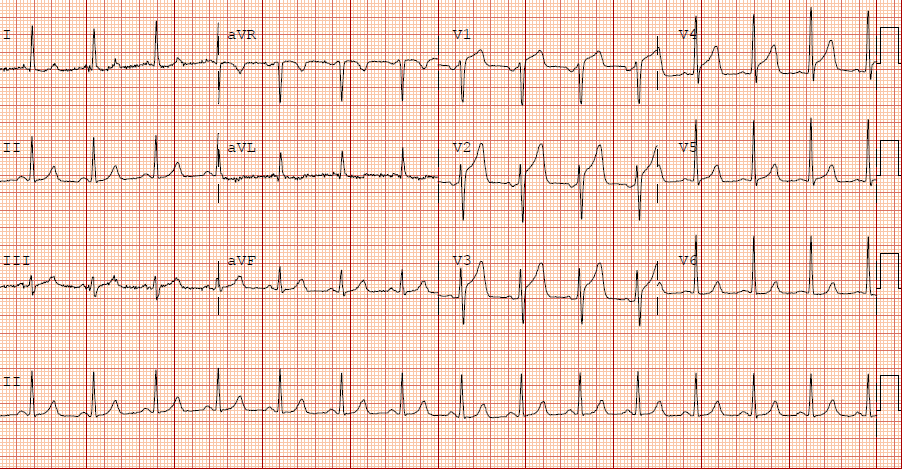 |
| QTc is 455 ms What do you think? |
Analysis
To me this is clearly an anterior STEMI, and it meets STEMI criteria even for someone under age 40 (at least 2.5 mm in V2 and V3, as measured at the J-point, relative to the PQ junction).
On the other hand, normal variant ST Elevation (often called early repolarization) may also have very marked ST elevation. So when there is upward concavity in all of V5-V6, absence of any ST depression, and absence of Q-waves, it still might be early repol and the computer might not call this anterior STEMI. Even the most contemporary algorithms are very inaccurate (see references below).
(which is not, as far as I know, programmed into automated interpretation algorithms):
You can find the calculator here:
--- (http://hqmeded-ecg.blogspot.com/p/rules-equations.html)
--- Or use the free iPhone app ("subtleSTEMI): https://itunes.apple.com/us/app/subtlestemi/id617146818?mt=8
---Or go to www.mdcalc.com: https://www.mdcalc.com/subtle-anterior-stemi-calculator
The QTc = 455
ST Elevation at 60 ms after the J-point (STE60V3) = 4mm
R-wave amplitude in V4 (RAV4) = 17 mm
QRS amplitude = 16.5
4-variable Formula value = 20.86. At greater than 18.2, this is diagnostic of LAD occlusion until proven otherwise.
Clinical Course
The computer did not diagnose STEMI. It did say "consider anterior injury." However, the physicians thought it was early repolarization and admitted the patient for rule out MI.
Serial troponins were all undetectable (Beckman Coulter Access AccuTnI+3 Troponin I on DXL 600), LoD 0.010 ng/mL, 99% reference at 0.040 ng/mL), and thus the patient did rule out for MI.
At some point, the symptoms resolved; it is unclear when.
Fortunately, they recorded a second ECG 12 hours after the first:
The physicians were alarmed by this and realized they may have dodged a bullet. They took the patient to the cath lab and found an 80% thrombotic LAD lesion. It was stented.
This patient (and his physicians) were very lucky. Had this patient not spontaneously reperfused, he would have lost his entire anterior wall, and possibly died.
It is dangerous to rely only on troponins for the diagnosis of acute coronary syndrome!
Learning Points:
1. Not all ischemic ST elevation results in elevated troponin
2. Unstable Angina still exists!! Troponins may all be negative even with severe ACS.
3. Use the formula
4. Serial ECGs should be every 15 minutes, NOT every 12 hours!
5. High sensitivity troponins might have made a difference. But maybe not.
6. Often, the only way to diagnose acute MI is with serial changes in the ECG. In this case, resolution of ST elevation was diagnostic even in the absence of troponin elevation.
References
Contemporary computer algorithms are insensitive (65%) for STEMI, and only approximately 90% specific:
4-variable Formula value = 20.86. At greater than 18.2, this is diagnostic of LAD occlusion until proven otherwise.
Clinical Course
The computer did not diagnose STEMI. It did say "consider anterior injury." However, the physicians thought it was early repolarization and admitted the patient for rule out MI.
Serial troponins were all undetectable (Beckman Coulter Access AccuTnI+3 Troponin I on DXL 600), LoD 0.010 ng/mL, 99% reference at 0.040 ng/mL), and thus the patient did rule out for MI.
At some point, the symptoms resolved; it is unclear when.
Fortunately, they recorded a second ECG 12 hours after the first:
 |
| Notice that all ST elevation has resolved! |
The physicians were alarmed by this and realized they may have dodged a bullet. They took the patient to the cath lab and found an 80% thrombotic LAD lesion. It was stented.
This patient (and his physicians) were very lucky. Had this patient not spontaneously reperfused, he would have lost his entire anterior wall, and possibly died.
It is dangerous to rely only on troponins for the diagnosis of acute coronary syndrome!
Learning Points:
1. Not all ischemic ST elevation results in elevated troponin
2. Unstable Angina still exists!! Troponins may all be negative even with severe ACS.
3. Use the formula
4. Serial ECGs should be every 15 minutes, NOT every 12 hours!
5. High sensitivity troponins might have made a difference. But maybe not.
6. Often, the only way to diagnose acute MI is with serial changes in the ECG. In this case, resolution of ST elevation was diagnostic even in the absence of troponin elevation.
References
Contemporary computer algorithms are insensitive (65%) for STEMI, and only approximately 90% specific:
1. Mawri S, Michaels A, Gibbs J, et al. The
Comparison of Physician to Computer Interpreted Electrocardiograms on
ST-elevation Myocardial Infarction Door-to-balloon Times. Critical Pathways in
Cardiology 2016;15:22-5.
2. Garvey JL, Zegre-Hemsey J, Gregg RE,
Studnek JR. Electrocardiographic diagnosis of ST segment elevation myocardial
infarction: An evaluation of three automated interpretation algorithms Journal
of Electrocardiology 2016;49:728-32.
Dear Dr Smith
ReplyDeleteHow frequent is this phenomena of NEGATIVE SERIAL TROP with Unstable Angina or Impending big Anterior STEMI as observed in the index case ?
Dr Rajiv Arora
Uncommon, but I've seen it many times. I have not found any papers on the topic. This was not only negative troponins, but UNDETECTABLE!!
DeleteIts possible in presence of Troponin Antibodies....such patients present with heart failure as well .. You should have sent tropinin antibodies ......google search for troponin antibodies .
DeleteIt would be interesting to know if this occlusion was distal to 1. diagonal but proximal
ReplyDeleteto 1. septal branch
Merci Dr Smith !
Al
Al, yes, it looks like it. Sometimes the septal perforator is distal to D1 and this is probably the case here, with occlusion distal to D1 (no STE in aVL, no STD in inferior leads) and proximal to S1 (large STE in V1)
DeleteMay I add that in the ECG#1 the anterior T waves are alarmingly large ("fat"), as I have lerned repeteadly in this blog?
ReplyDeleteMany thanks for presenting this case!
Mario, of course. And that is why the QTc is longer than one would find in normal variant. It is the long QT that drives the formula to a high value.
DeleteSteve
the alternative to diagnose ischemic injury could be the administration of nitrates and the observation of the response in the pz?
ReplyDeleteNot sure what you are saying
DeleteWonderful case by Dr. Smith! I’ll add the following comments: i) I would not be expecting “Early Repolarization” as the explanation for this ECG in a man who is 58 and presenting with active chest pain at the time of this tracing (ie, early repol must be a diagnosis of exclusion in a patient this age presenting with active chest pain … ); ii) Although concave-up ST elevation may be seen in various lead areas when due to “early repolarization” — it is NOT typical to see 3mm of J-point ST elevation in lead V1, but none in inferior or lateral leads; iii) Early repol does not typically present with the “shape” of ST-T wave that we see in all anterior leads (more than 3mm of J-point ST elevation with disproportionately tall, peaked T waves); and iii) if this was pure “early repolarization” — I would NOT expect to see the FLAT ST segment that we clearly see in lead V6 … LOTS to learn from this case — THANKS to Dr. Smith for presenting!
ReplyDeleteThanks, Ken!
DeleteDr. Smith:
ReplyDeleteThe first ECG showed STEMI, which implied 100% occluded LAD. I wonder if it is possible that the thrombus could be spontaneously lysed from 100% to 80%? Or, it was the 80% occluded LAD that could manifest as ''ST elevation'' in lead V1 to V4? And, if it was LAD spontaneously lysed from 100% to 80%, why there was no reperfusion T waves like the mechanism of Wellen's syndrome?
Thanks again for presenting this case!
Allen,
DeleteIt spontaneously lysed from 100% to 80%, and did so fast enough that there was no myocardial necrosis (no elevated troponin).
Wellens' waves only occur when there is some infarction, often very little. But with no troponin elevation, one does not expect Wellens' waves.
STeve
Would cath lab accepts initial ecg as stemi? if not, would echo with anterior akinesia convince unterventionist?
ReplyDeleteEvery interventionalist is different! Echo would definitely be convincing.
DeleteGood case. Nondetectible troponins define a subgroup with stable or relatively stable plaque and/or short CA spasm occuring spontaneously or inducible by activity, eating, anxiety, et. al. Patients with obstructive stable angina also have provocative ST elevation, positive NSTs, positive stress echos but usually without sufficient tournicut time for myocardial cell injury and enzyme release, ie, nondetectable or < 99% gender based cut-off troponins. The literature seems to support primarily medical management for this group. A new anginal pattern or rest angina relegates this patient into an unstable category.
ReplyDeleteMedical management is not appropriate for ruptured plaque with thrombus, which is what was found here. A stent is necessary.
Delete