
This was sent by Nick Jubert, MD, one of our fine EM residency graduates who works at a facility without a cath lab, so has to transfer patients who need a cardiac cath:
I immediately activated the cath lab given concern for left main vs LAD. Further history from paramedics was she had blood pressure of 103/70, they gave the patient ASA and nitroglycerin. After nitroglycerin, the blood pressure dropped into the 80s.
Steve,
Really interesting case I saw this morning, thought I’d send it your way.
Case
Case
A 60 year old female with a history of HTN, DM, hyperlipidemia presented via EMS with crushing central chest pain radiating to her neck, 7/10. Here is the EMS EKG:
 |
| There is RBBB, with ST elevation in aVR and V1, and diffuse, marked, ST depression in I, II, aVF, aVL and V3-V6. This is severe subendocardial ischemia. |
I immediately activated the cath lab given concern for left main vs LAD. Further history from paramedics was she had blood pressure of 103/70, they gave the patient ASA and nitroglycerin. After nitroglycerin, the blood pressure dropped into the 80s.
On arrival she looked terrible. Pale, diaphoretic, scared. HR 109, BP 65/53. Peripheral pulses intact including DP, and radial bilaterally. We repeated the EKG and got the above. We obtained IV access, gave IV fluid bolus, heparin bolus, withheld P2Y12 inhibitors due to concern for need for surgery, and started dopamine drip (cardiology asked for this specifically). She became bradycardic in to the 30’s and I gave atropine 1mg, which she responded well to, and she was transferred for emergent cath.
When she got to the referral hospital, she was brought to the cath lab, had clean arteries but had a large shunt from aorta into the right atrium from acute sinus of valsalva rupture. She had a known history of sinus of valsalva aneurysm, but given the EKG, I felt I had a good reason for her to be hemodynamically unstable given my concern for a large territory of infarction plus she was given nitroglycerin. I did not ultrasound her because I did not want to delay her transfer. Is there anything in the above EKG that could have given some clue to this as a cause? Obviously in retrospect, I wish I had just taken the time to ultrasound her heart, given the limited images I can see from her chart, I likely would have identified the large defect and seen hyper dynamic cardiac function which would not have fit her clinical picture.
She had an aortic balloon pump placed and has now gone for surgical repair, intubated, on heparin, NE and dopamine drips. Interesting case.
Questions and Answers:
Is there anything in the above EKG that could have given some clue to this as a cause?
One's initial reaction to the case is severe ACS!! However, the ECG shows ischemia. It does NOT show the etiology of ischemia. I have stated many times on this blog that diffuse subendocardial ischemia is more often caused by supply demand mismatch than by ACS. I have demonstrated that ST elevation in aVR is NOT caused by Left Main occlusion, a false claim which is even made in the ACC/AHA STEMI guidelines. [ST Elevation in Lead aVR, with diffuse ST depression, does not represent left main occlusion, see quote from the blog post below (1)]
Your solution is exactly right. Had you looked with ultrasound, you would have seen hyperdynamic function and that would have made ACS extremely unlikely. Combined with the history of sinus of valsalva aneurysm, the diagnosis might have been made earlier. Fortunately, (it seems) she did well. In any case, sounds like great management. Auscultation of a loud murmur may have tipped you off as well. But we all know how difficult it is to appreciate a murmur in a loud ED.
Rupture of Sinus of Valsalva Aneurysm
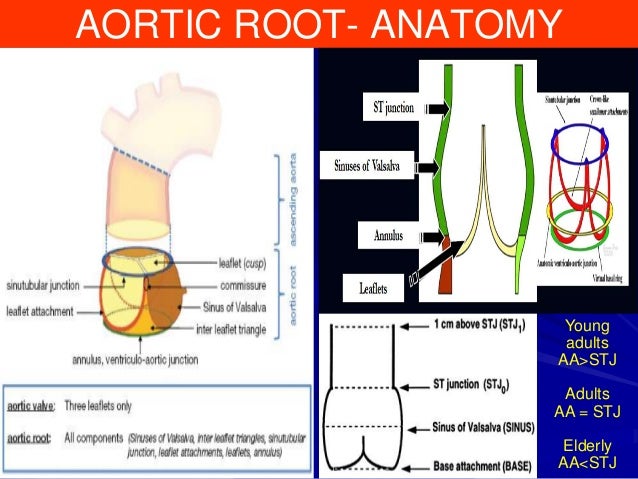
The sinuses of Valsalva are any one of the pouches of the aorta and pulmonary artery which are located behind the flaps of the semilunar valves and into which the blood in its regurgitation toward the heart enters and thereby closes the valves; it is also called the aortic sinus. Most ruptures of the sinus of Valsalva are indolent, small, and without acute symptoms. An anatomic etiology of symptoms may be suspected with heart auscultation (murmur), and diagnosis is made by a routine echocardiogram or, if the patient is suspected of having coronary disease as the etiology of symptoms, an angiogram. But some are sudden and life threatening, such as this one. They are usually aneurysms of the right coronary sinus, and most commonly rupture into the RV, then the right atrium (as in this case).
It is difficult to find any description of cases of such acute severity.
Here are some large case series:
Rupture of Sinus of Valsalva Aneurysm
The sinuses of Valsalva are any one of the pouches of the aorta and pulmonary artery which are located behind the flaps of the semilunar valves and into which the blood in its regurgitation toward the heart enters and thereby closes the valves; it is also called the aortic sinus. Most ruptures of the sinus of Valsalva are indolent, small, and without acute symptoms. An anatomic etiology of symptoms may be suspected with heart auscultation (murmur), and diagnosis is made by a routine echocardiogram or, if the patient is suspected of having coronary disease as the etiology of symptoms, an angiogram. But some are sudden and life threatening, such as this one. They are usually aneurysms of the right coronary sinus, and most commonly rupture into the RV, then the right atrium (as in this case).
{kind=link}
It is difficult to find any description of cases of such acute severity.
Here are some large case series:
Sinus of Valsalva Aneurysms—47 Years of a Single Center Experience and Systematic Overview of Published Reports
http://www.heartcenter.org.tw/ch/wp-content/uploads/2015/02/2004-Ruptured-Congenital-Sinus-of-Valsalva-Aneurysms.pdf
(1) Quote from the above blog post: This is even stated in the lastest 2013 ACC/AHA STEMI guidelines (O’Gara PT et al. JACC 61(4):e83; January 29, 2013). However, the guidelines use as evidence an article by Jong et al. (Int Ht J 2006; 47(1):13-20). That article misleadingly defines "occlusion" as any stenosis greater than 50%, when it should rather be defined as 100%, or nearly so.
Although off the point, I am frequently embarrassed by how relatively little I know about reading EKGs. So .....I believe an intra-aortic balloon pump would be relatively contraindicated with a left-to-right shunt.
ReplyDeleteNot sure, but balloon pumps only support diastolic pressure, and this is critical for coronary perfusion. The coronary perfusion here is not good. Seems to me that the biggest problem is diastolic hypotension, NOT left to right shunt with hypoxia.
DeleteInteresting case. Would you comment on V1 mild ST elevation, compared to low ST in V2, plus RBB appearance, plus unspecific tachy, related to a RV strain from left to right shunting, and about a possible Ddx of PE (I guess unstable RV isolated infarct won’t produce all this). I guess massive low ST + AVR elevation would probably not be explained just by PE. Many thanks!
ReplyDeleteAlain,
DeleteThe doc did not mention the presence or absence of hypoxia. The best way to differentiate this pathology from PE would be oxygenation: if PE, then there would be clear lungs with hypoxia. If not PE, there would EITHER be no hypoxia, OR there would be hypoxia AND pulmonary edema. In both cases, the LV could be hyperdynamic, but in PE the RV would not be hyperdynamic. The RV should be hyperdynamic in this ruptured aneurysm case. Also, this case should have had a loud murmur.
So the ECG alone will not give the answer.
only in combination with clinical data.
Steve
Paramedics should not give nitroglycerin if BP is 100/70 mmhg and there is no two peripheral venous access with fluid boluss prior that. Patient became unstable. Why paramedics did not gave morphine and heparin to the patient...
ReplyDeleteAigars,
DeleteI agree Nitro not indicated. But morphine is of no use. And also dangerous.
Steve
GREAT case. Thanks for presenting!
ReplyDelete