
Case 1.
A younger middle-aged male called EMS for chest pain. They recorded a prehospital ECG which I do not have, but they did a prehospital cath lab activation for chest pain and inferolateral ST elevation.
Here is the ED ECG:
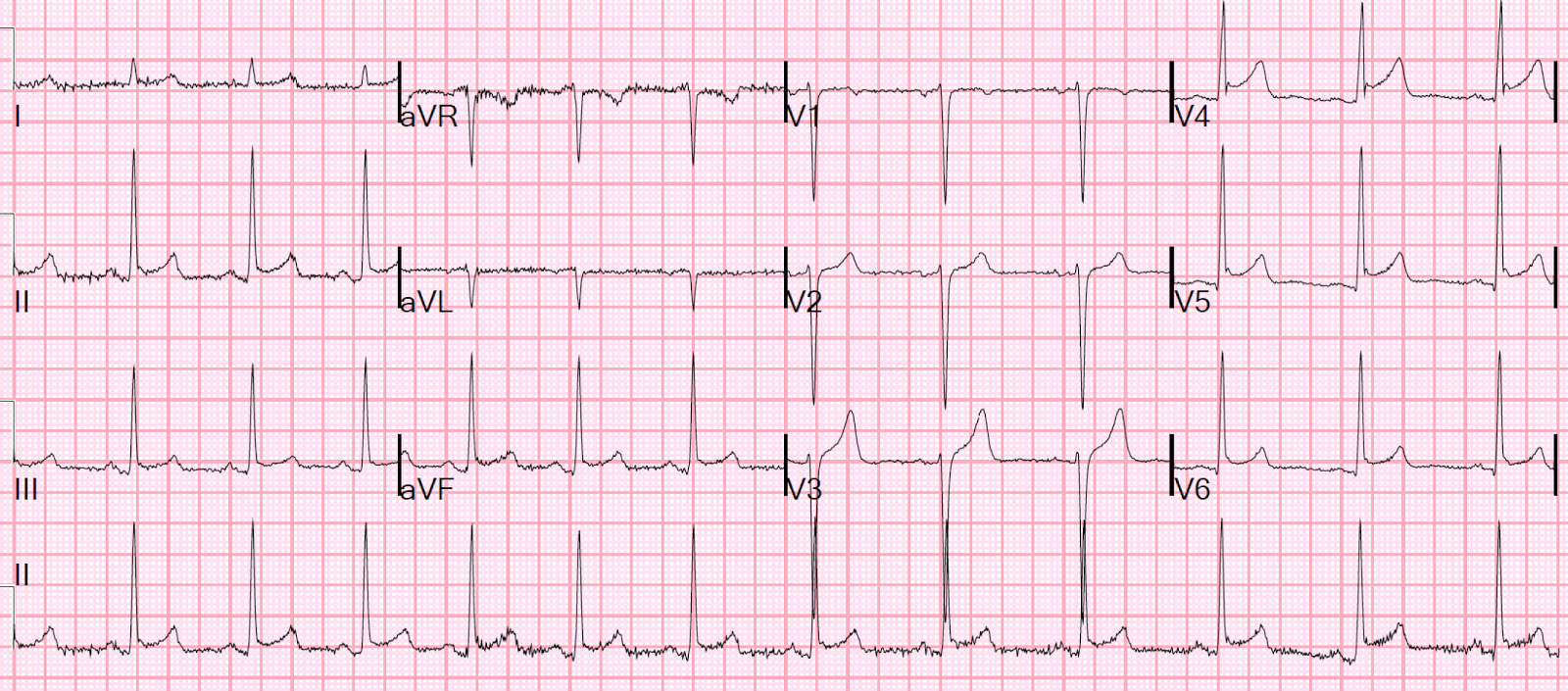 |
There is inferior ST elevation and also ST elevation in V5 and V6.
Is this inferior and lateral STEMI?
|
Case 2.
A middle-aged male presented with chest pain:
 |
| There is inferior ST elevation and also ST elevation in V5 and V6. Is this inferior and lateral STEMI? |
Case 1 is typical early repolarization. A stat echo was negative, the cath lab was cancelled, and serial ECGs were negative. Other aspects which strongly suggest early repol are: 1) high voltage in leads with ST elevation; 2) proportionally small T-waves and ST elevation in these leads.
Case 2 is typical pericarditis (and was, indeed, proven pericarditis). The absence of reciprocal ST depression in lead aVL makes it very unlikely to be inferior MI, even when there is ST elevation in V5 and V6.
Learning point: The absence of reciprocal ST depression in lead aVL makes it very unlikely to be inferior MI, even when there is ST elevation in V5 and V6.
But wouldn't there always be ST elevation in aVL if there is STE in V5 and V6?
No!
V5 and V6 are lower down and more like lead II than like aVL.
Case 3.
This patient presented with one hour of chest pain.
 |
| The diagnosis of inferior-posterior-lateral STEMI is obvious, but look at the huge ST elevation in V5 and V6. Nevertheless, there is a small amount of reciprocal ST depression in lead aVL. |
With such high ST elevation in V5 and V6, wouldn't you expect an absence of ST depression in lateral lead aVL, or even ST elevation in aVL?
No!
We found in our study of inferior MI (http://www.ajemjournal.com/article/S0735-6757(15)00818-9/abstract) that: of patients whose ECGs had inferior ST elevation due to STEMI and also had ST elevation in V5 and V6, 35 out of 35 (100%!) had some ST depression in lead aVL.
This is helpful in cases such as these:
 |
| There is inferior ST elevation and also ST elevation in V5 and V6. However, there is no reciprocal ST depression in aVL. This was early repolarization. |
 | |
|
If there is inferior ST elevation, but no reciprocal ST depression in aVL, you should be skeptical of the diagnosis of STEMI even if there is ST elevation in V5 and V6.
Case 1 st/t ratio in V6 is more then 25% also some pr depression. Did viral pricarditis r/o?
ReplyDeleteThe 25% rule is not reliable. See the last two ECGs--these are also early repol. PR depression up to 0.8 mm is also normal (normal atrial repolarization wave). Case 1 is a typical ECG of an asymptomatic patient with ST elevation (i.e., early repol); it is classic for early repol. I think many patients with chest wall pain and early repol are wrongly given the diagnosis of pericarditis.
DeleteHas the 25% rule been proven wrong with published data, or is it your personal observations.Cheers!
DeleteHere is the original study: http://circ.ahajournals.org/content/65/5/1004.full.pdf
DeleteIt could not be validated: https://www.researchgate.net/profile/Ravindra_Bhardwaj/publication/229426436_Differential_Diagnosis_of_Acute_Pericarditis_From_Normal_Variant_Early_Repolarization_and_Left_Ventricular_Hypertrophy_With_Early_Repolarization_An_Electrocardiographic_Study/links/546b92e90cf2397f7831c449.pdf
There was lots of overlap.
You'll see that their examples of pericarditis do NOT have J-waves. The examples of early repol do have J-waves.
In the validation, the ST/S ratio in lead I > 0.25 turned out to be the best in this validation. But even that was only 65% specific for pericarditis. Not very good.
Steve
thanks Steve!
DeleteOK . What method do you use to DD early repo from pricarditis (mild) for sure? Thanks dr smith
ReplyDeleteECG: 1) deeper PR depression 2) absence of J-waves 3) Spodick's sign (notice the case of pericarditis above has Spodick's sign (descending TP segment). I am not terribly confident in Spodick's sign especially since Amal Mattu has told me he conducted a good study of this and it was negative (so far unpublished, even as abstract)
DeleteI don't think the ECG is the best way. Other clinical info is important: 1) absence of chest wall tenderness 2) friction rub 3) pericardial effusion
Finally, if you don't have the above, who cares? The important diagnosis is STEMI or not and, if pericarditis, is there an effusion? Otherwise, pericarditis and chest wall pain are simply painful but benign conditions. If you have a high suspicion of pericarditis, maybe you want to add colchicine.
thanks
DeleteHi,
ReplyDeleteWas your study (on reciprocal ST depression in aVL) limited to RCA and LCX lesions ? I am asking because LAD lesions including D1 but not S1 produce widespread ST elevation with ST elevation in aVL and inferior STE (in addition to anterior STE). These pose the the real problem differentiating STEMI vs. pericarditis (and vs. Early repol). Any data or comments on this?
Thanks in advance
This comment has been removed by the author.
DeleteEmre,
DeleteLAD or D1 lesions rarely cause STE in aVL and inferior leads. They frequently cause STE in aVL with ST depression in inferior leads.
There are some exceptions
STeve