
I posted this on March 1, 2012. I was inspired by a post by Len Jin Yee to repost. But this time without the answers. These are all on a theme, which will quickly become obvious.
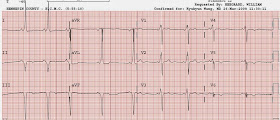
Case 1. A patient presented with an irregular and fast wide complex tachycardia and was electrically cardioverted. Here is the post cardioversion ECG:
This is WPW with secondary repolarization abnormalities. Notice the very short PR interval and the delta waves, best seen in leads V5 and V6. This mimics both anterior STEMI and/or left bundle branch block.
This patient turned out to have Ebstein's anomaly, (a description of which is beyond the scope of this blog) with WPW.
_______________________________________________________________________
Case 2. A patient with chest pain
In this case, WPW mimics inferior and posterior MI. There was no superimposed MI of any age. Note that there are Q-waves in II, III, aVF and that the T-wave in these leads is upright. In a study of 50 patients with inferior Q-waves due to WPW and not due to MI, 47 had an upright T-wave. The author, Ary Goldberger, suggests that in the presence of a delta wave and Q-wave, the T-wave should be discordant (opposite the Q-wave) as it is in this case, or at least isoelectric. He suggests that if it is concordant, then one should suspect inferior infarction. Accordingly, lateral QRS and T-wave should also be discordant.
Other than the study on inferior Q-waves and its implications for diagnosis of inferior MI, I know of no other studies assessing this phenomenon. I am not sure if, in WPW, there is a predictable pattern. Are the QRS and ST-T complex normally concordant or discordant? Not sure.
_______________________________________________________________________
Case 3: A patient with chest pain
I think you are catching on that WPW can mimic acute STEMI, with ST elevation and ST depression. However, if you remember to always evaluate ST elevation and depression in the context of the QRS, and the abnormal depolarization results in abnormal repolarization, you will look at the QRS and recognize how abnormal it is: wide, with short PR interval and delta waves. The ST-T abnormalities are secondary to the WPW, not primary.
_____________________________________________________________________
Case 4. A patient with chest pain
Wrong!! This patient has acute inferior STEMI superimposed on baseline WPW. There is simply too much ST elevation for this to be due to WPW alone. Here is his baseline ECG for comparison.
____________________________________________________________________
Case 5. A male in his 50's presents with 1.3 hours of chest pain.
14 minutes later, this was recorded:
Neither of these ECGs, in my opinion, clearly show ischemia because WPW can so often mimic ischemia. However, perhaps simply because of worrisome symptoms, or perhaps because they were unaware that these ST-T repolarization changes can be entirely due to WPW, the clinicians took the patient for an angiogram, which showed a 95% stenosis of the first diagnonal with TIMI 2 flow. It was stented.
8 hours later, post reperfusion, this was recorded:
Day 2 ECG: (troponin I peaked at 32 ng/mL)
Day 3, after ablation of the accessory pathway:
Summary
WPW has abnormal depolarization through a bypass tract, manifesting as a delta wave. And like other ECG abnormalities that have abnormal depolarization (LVH, LBBB, RBBB, Brugada, hyperkalemia, and others), they also have abnormal repolarization. "Secondary repolarization abnormalities." (Not primary, meaning the QRS is normal but repolarization is abnormal, as in ischemia).
Above I showed 5 cases:
Cases 1-3 are of WPW with secondary repolarization abnormalities that could mimic old or acute MI.
Case 4 shows a baseline WPW, then with MI superimposed on it.
Case 5 is a case in which WPW conceals acute MI.
Learning points:
1. WPW alters both depolarization and repolarization and can both mimic and obscure acute MI.
2. In WPW with inferior Q-waves (but without new or old MI), the T-wave is usually upright (discordant).
3. In WPW with inferior Q-waves, a concordant T-wave should raise suspicion for MI, either old or new.
4. I am uncertain as to whether there are other concordance and discordance rules that may help decipher ischemia in the presence of WPW.
Case 1. A patient presented with an irregular and fast wide complex tachycardia and was electrically cardioverted. Here is the post cardioversion ECG:
 |
| What is going on? See below. |
This is WPW with secondary repolarization abnormalities. Notice the very short PR interval and the delta waves, best seen in leads V5 and V6. This mimics both anterior STEMI and/or left bundle branch block.
This patient turned out to have Ebstein's anomaly, (a description of which is beyond the scope of this blog) with WPW.
_______________________________________________________________________
Case 2. A patient with chest pain
 |
| Is it inferior-posterior MI, whether acute or old? There appear to be inferior Q-waves with possible hyperacute T-waves, reciprocal T-wave inversion in aVL suggestive of inferior MI. There are tall right precordial R-waves with ST depression and T-wave inversion suggestive of concomitant postererior MI. See below. |
In this case, WPW mimics inferior and posterior MI. There was no superimposed MI of any age. Note that there are Q-waves in II, III, aVF and that the T-wave in these leads is upright. In a study of 50 patients with inferior Q-waves due to WPW and not due to MI, 47 had an upright T-wave. The author, Ary Goldberger, suggests that in the presence of a delta wave and Q-wave, the T-wave should be discordant (opposite the Q-wave) as it is in this case, or at least isoelectric. He suggests that if it is concordant, then one should suspect inferior infarction. Accordingly, lateral QRS and T-wave should also be discordant.
Other than the study on inferior Q-waves and its implications for diagnosis of inferior MI, I know of no other studies assessing this phenomenon. I am not sure if, in WPW, there is a predictable pattern. Are the QRS and ST-T complex normally concordant or discordant? Not sure.
_______________________________________________________________________
Case 3: A patient with chest pain
+anterior+STE+-+cropped.jpg) |
| There is anterior ST Elevation (V1, V2) with ST depression in inferior and lateral leads. Looks like a septal STEMI, right? |
I think you are catching on that WPW can mimic acute STEMI, with ST elevation and ST depression. However, if you remember to always evaluate ST elevation and depression in the context of the QRS, and the abnormal depolarization results in abnormal repolarization, you will look at the QRS and recognize how abnormal it is: wide, with short PR interval and delta waves. The ST-T abnormalities are secondary to the WPW, not primary.
_____________________________________________________________________
Case 4. A patient with chest pain
 | ||||||
| Again, there are delta waves with subsequent inferior ST elevation and reciprocal ST depression in I and aVL, as well as V2. You are now tuned into this, and realize that the ST elevation is secondary to the WPW, right? |
Wrong!! This patient has acute inferior STEMI superimposed on baseline WPW. There is simply too much ST elevation for this to be due to WPW alone. Here is his baseline ECG for comparison.

____________________________________________________________________
Case 5. A male in his 50's presents with 1.3 hours of chest pain.
 |
| Clearly there is WPW, with short PR interval and delta waves. There are deep QS-waves (negative delta waves) in III and aVF, with concordant T-waves. T-waves are upright in I and aVL. Is there old or new inferior MI? There is ST depression in V3-V6. There are nonspecific ST and T-wave findings in V4-V6. Are these all due to WPW, or is there something hiding? |
14 minutes later, this was recorded:
 |
| Minimal changes |
Neither of these ECGs, in my opinion, clearly show ischemia because WPW can so often mimic ischemia. However, perhaps simply because of worrisome symptoms, or perhaps because they were unaware that these ST-T repolarization changes can be entirely due to WPW, the clinicians took the patient for an angiogram, which showed a 95% stenosis of the first diagnonal with TIMI 2 flow. It was stented.
8 hours later, post reperfusion, this was recorded:
 |
| Many T-waves are now flattened or inverted. |
Day 2 ECG: (troponin I peaked at 32 ng/mL)
 |
| Inferior T-waves are now clearly upright, lateral T-waves clearly inverted. So these discordant T-waves in III and aVF, and I and aVL appear to be the normal discordant T-waves that one finds when there are inferior Q-waves due to WPW. This appears to be a case of pseudonormalization of T-waves, but it is not true pseudonormalization because it is not from re-occlusion, but rather from reperfusion. In other words, after reperfusion, the T-wave vectors are in the expected direction for WPW, not inverted from normal as is common in reperfusion. |
Day 3, after ablation of the accessory pathway:
.png) |
| QRS is normalized except for Q-waves in I and aVL (due to the lateral AMI suffered on this occasion). Interestingly, the T-waves are inverted in III and aVF, but not in I and aVL; that is to say that there are apparently no lateral reperfusion T-waves. There are large T-waves in V2 and V3 which may represent posterior reperfusion T-waves (or early repol, but without a comparison from prior non-WPW ECG, this is uncertain). |
Summary
WPW has abnormal depolarization through a bypass tract, manifesting as a delta wave. And like other ECG abnormalities that have abnormal depolarization (LVH, LBBB, RBBB, Brugada, hyperkalemia, and others), they also have abnormal repolarization. "Secondary repolarization abnormalities." (Not primary, meaning the QRS is normal but repolarization is abnormal, as in ischemia).
Above I showed 5 cases:
Cases 1-3 are of WPW with secondary repolarization abnormalities that could mimic old or acute MI.
Case 4 shows a baseline WPW, then with MI superimposed on it.
Case 5 is a case in which WPW conceals acute MI.
Learning points:
1. WPW alters both depolarization and repolarization and can both mimic and obscure acute MI.
2. In WPW with inferior Q-waves (but without new or old MI), the T-wave is usually upright (discordant).
3. In WPW with inferior Q-waves, a concordant T-wave should raise suspicion for MI, either old or new.
4. I am uncertain as to whether there are other concordance and discordance rules that may help decipher ischemia in the presence of WPW.
I was wondering if you would really mistake the first 3 ecg's for mi if you wouldn't know about wpw. My brain told me to see a bbb on first sight.
ReplyDeleteWe would have to try it out on some people to know exactly how many it would fool, but they all fooled some people and I would bet that many would think they are MI.
Delete