
Case 1.
A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chest pain with radiation to the anterior neck, with associated nausea. She had known HTN and DM. She appeared to be in distress. She was given sublingual NTG with improvement, but there was not complete resolution.
Here was here initial ECG:
There was an old ECG for comparison:
A bedside cardiac ultrasound was done by the emergency physician. Here is the parasternal short axis view:
There is an anterior and lateral wall motion abnormality.
This still helps to show the wall motion abnormality:
The Cath Lab was activated, and here are the results:
1. LM: No significant stenosis.
2. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis. (Culprit, stented)
3. LCX: Luminal irregularities, no significant stenosis. Two OM branches without significant stenosis.
4. RCA: dominant. Luminal irregularities without significant stenosis. Supplies a small RPDA and RPLA.
This was the post-cath ECG:
A large Diagonal artery may supply both the lateral wall and part of the anterior wall.
He was given aspirin, clopidogrel, IV nitroglycerine, and heparin, the general cardiologist was called and notified that this patient was very high risk and needed close attention. He readily agreed, and the plan was to admit for close observation, serial ECGs and troponins, and to scrutinize for any recurrence of pain or change in the ECG.
The first troponin I then returned at 0.063 ng/ml (upper limit of normal = 0.025 ng/ml). Repeat ECG remained unchanged.
--He remained pain free and the plan remained to admit with a diagnosis of Non-STEMI on medical therapy with plan for angiogram in the morning.
--Just before admission to the hospital, the patient admitted to recurrent pain and appeared uncomfortable. Therefore, the cath lab was activated urgently.
--The suspicion was for a circumflex (or obtuse marginal branch) or diagonal artery occlusion or subtotal occlusion.
--At cath, there was a 95% proximal LAD stenosis with TIMI-II flow, proximal to a large diagonal. A stent was placed and the patient became pain free.
Lessons:
When there is ST elevation in aVL, with reciprocal ST depression in III:
1. Look for:
a. J-waves
b. Other ST depression
c. Large T-waves
d. Symmetric T-waves
e. Down-Up T-waves
2. Compare with an old ECG
3. Use ED Echo if available
4. Use formal Echo
5. A positive troponin is helpful (a negative one is not)
A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chest pain with radiation to the anterior neck, with associated nausea. She had known HTN and DM. She appeared to be in distress. She was given sublingual NTG with improvement, but there was not complete resolution.
Here was here initial ECG:
 |
| There is ST elevation in I and aVL, with inferior reciprocal ST depression in all of II, III, and aVF, and a down-up T-wave in aVF (a sign that is very specific for ischemia). There is also ST depression in V3-V6. This ECG is diagnostic of ischemia. |
It is important to compare this one with the false positive case #3 at the bottom; that one is a case which could fool you.
There was an old ECG for comparison:
 |
| One year prior with no ST segment abnormalities |
A bedside cardiac ultrasound was done by the emergency physician. Here is the parasternal short axis view:
There is an anterior and lateral wall motion abnormality.
This still helps to show the wall motion abnormality:
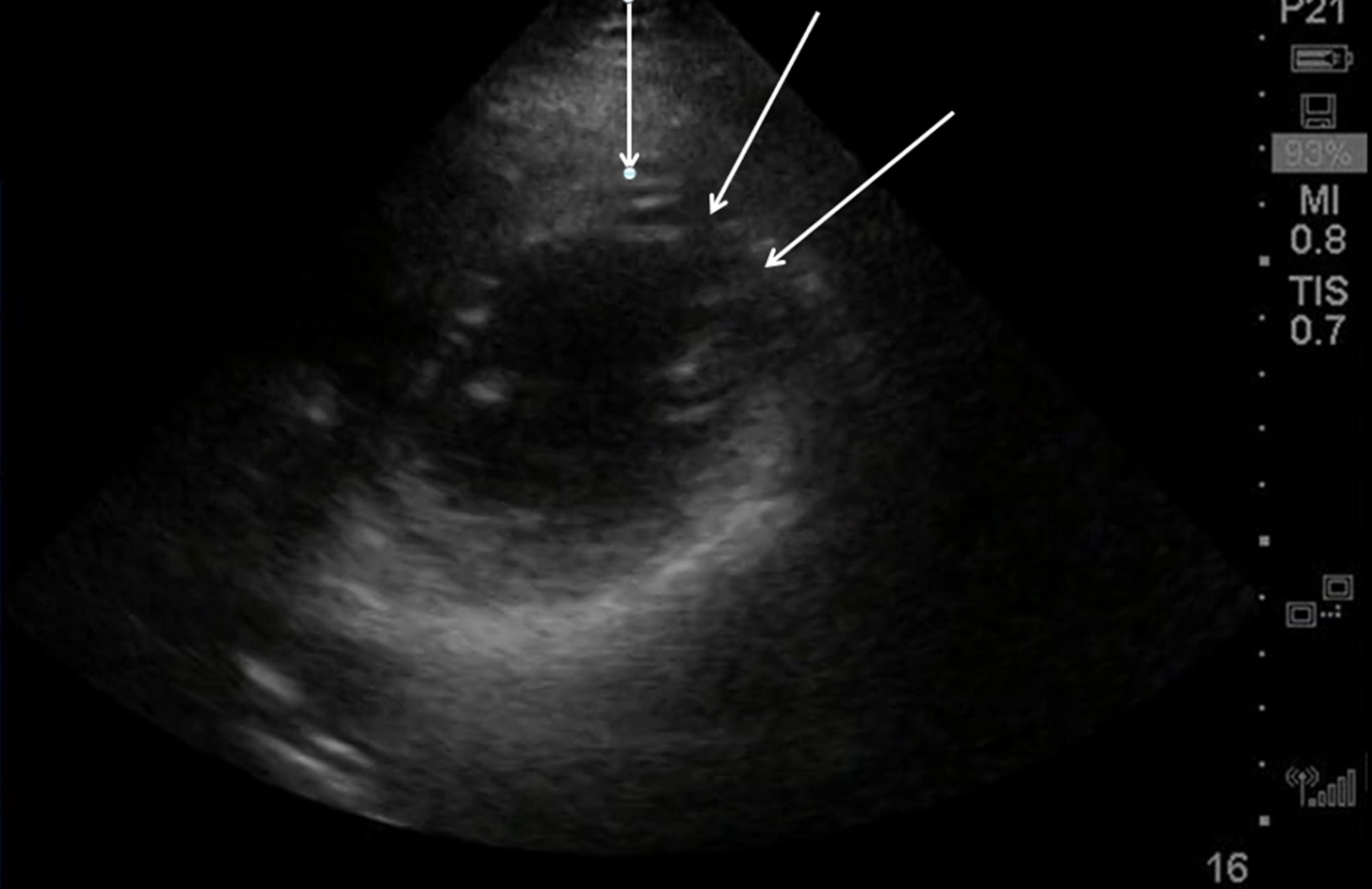 |
| Arrows point to area of wall motion abnormality |
The Cath Lab was activated, and here are the results:
1. LM: No significant stenosis.
2. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis. (Culprit, stented)
3. LCX: Luminal irregularities, no significant stenosis. Two OM branches without significant stenosis.
4. RCA: dominant. Luminal irregularities without significant stenosis. Supplies a small RPDA and RPLA.
After cath lab activation, her initial troponin returned at 0.124 ng/mL (99% level = 0.030 ng/mL)
 |
| After reperfusion: aVL shows resolution of ST elevation and inverted (reperfusion) T-wave. There is also some terminal T-wave inversion in anterior precordial leads |
A large Diagonal artery may supply both the lateral wall and part of the anterior wall.
Case 2: Another subtle lateral MI, from this post:
A male in his 60's presented 30 minutes after the onset of crushing substernal chest pain. Medics recorded 2 ECGs, one before and one after sublingual NTG, and both are similar to the first ED ECG. The patient had never had pain like this before. The pain improved from 9/10 to 3/10 after NTG. Here is the initial ED ECG:
 |
| There is subtle ST elevation in I and aVL with subtle reciprocal ST depression in III. Look at aVF. There is a downsloping reciprocal ST segement followed by an upright T-wave ("down-up" T-wave). This morphology is highly suspicious for ischemia. There are also symmetric anterior T-waves with very poor R-wave progression. T-waves in V4-V6 are taller than normal (compare to ECG in case 3 below) |
This ECG, especially along with the very typical
history, was very worrisome, but not absolutely diagnostic of, ischemia.
Several serial ECGs showed no change, even after the pain finally resolved to
0/10 after NTG.
He was given aspirin, clopidogrel, IV nitroglycerine, and heparin, the general cardiologist was called and notified that this patient was very high risk and needed close attention. He readily agreed, and the plan was to admit for close observation, serial ECGs and troponins, and to scrutinize for any recurrence of pain or change in the ECG.
The first troponin I then returned at 0.063 ng/ml (upper limit of normal = 0.025 ng/ml). Repeat ECG remained unchanged.
--He remained pain free and the plan remained to admit with a diagnosis of Non-STEMI on medical therapy with plan for angiogram in the morning.
--Just before admission to the hospital, the patient admitted to recurrent pain and appeared uncomfortable. Therefore, the cath lab was activated urgently.
--The suspicion was for a circumflex (or obtuse marginal branch) or diagonal artery occlusion or subtotal occlusion.
--At cath, there was a 95% proximal LAD stenosis with TIMI-II flow, proximal to a large diagonal. A stent was placed and the patient became pain free.
Case 3: False positive
And here is a similar one that is NOT MI. How do we tell the difference?
 |
| There is ST elevation in I and aVL, with reciprocal ST depression in lead III. |
Just so you don't think I'm cheating by using a retrospectoscope, this was sent to me without any outcome, and I read it as "no MI" with a high degree of certainty. This is because:
1. The remainder of the ECG is normal. No poor R-wave progression, no other ST depression, no symmetrical T-waves, no large T-waves, no down-up T-waves, typical early repol in anterior leads
2. The reciprocal ST depression is in lead III only. Not in leads II and aVF.
3. There are distinct J-waves in the two leads with ST elevation. This is highly suggestive of early repolarization in these leads.
4. The T-waves in I and aVL are not large (this was also true with the MI case 1 at the top, but that case had many other suspicious findings (many leads with ST depression and no J-waves)
When there is ST elevation in aVL, with reciprocal ST depression in III:
1. Look for:
a. J-waves
b. Other ST depression
c. Large T-waves
d. Symmetric T-waves
e. Down-Up T-waves
2. Compare with an old ECG
3. Use ED Echo if available
4. Use formal Echo
5. A positive troponin is helpful (a negative one is not)
Thanks Dr.Smith.. Feels like STEMI but the ST elevation is less than 1mm for tPA to be given. the Echo is very clear regarding the lateral regional wall abnormality. Would that in combination (ECG, ECHO) be a reason to administer tPA if pci not available ? or i would call it NSTEMI?
ReplyDeleteThat is an incredibly complex question with no good answer. All depends on risk/benefit. ST elevation is arbitrary and the studies establishing the efficacy of tPA were crude. ST elevation of 1 mm is a very poor criterion for significant coronary occlusion, has poor sensitivity, specificity. Studies generally had mortality as the outcome and even inferior STEMI had little mortality benefit from tPA. For regulatory purposes, this is a NonSTEMI and door to needle and door to ballloon standard measures should not apply. But it really is ischemic ST elevation due to coronary occlusion. tPA, if it works, will potentially save a significant amount of myocardium, but is it worth the risk of intracranial hemorrhage? That is a tough question. The alternative is to give aspirin, a P2Y12 inhibitor, heparin or LMWH, and a GPIIbIIIa inhibitor such as eptifibatide, then transfer to nearest PCI facility. All depends on the risk as well as the benefit. I might give half dose tPA instead of eptifibatide, then transfer.
DeleteSee this article: http://interventions.onlinejacc.org/article.aspx?articleid=1110256
Steve Smith
In case 3, what is the likely explanation for the STD in lead III and the flatness in aVF?
ReplyDeleteThe ST elevation axis of this early repol is directly at 0 degrees, toward lead I. Lead aVF, then, is 90 degrees to this ST vector and thus has no ST shift. Lead III is therefore 120 degrees away from the ST vector and therefore has a bit of reciprocal ST depression
DeleteDear Dr Smith,
ReplyDeletethank you for again a wonderful case.
In case 3, how would you interpret the straight T-waves in the anterior leads.
I learned to also look at the morfology of the T waves, and V2V3V4 seem worrisome to me.
Any idea's on the sensitivity / specificity of this perticular finding?
Kind regards,
Kris
Kris,
DeleteYes, at first glance, these are worrisome. however, the QTc was relatively short and the R-wave amplitude is good. If you know of my LAD vs. early repol equation, you can use it to assess whether the ST elevation in V2-V4 is ischemic or not. (see the side bar for the excel applet). I do not have the computerized QTc for this image, but it is quite short, at most about 370ms. The resulting number would be quite low.
Where are you writing from? Interesting photo next to your name! Looks like the Alps.
Steve Smith
And also another point I see is 11mm in aVL, is that also worthnoting?
ReplyDeleteYes, it is, Martin. Thanks!
DeleteSteve
This comment has been removed by a blog administrator.
ReplyDeleteLooking at the first case I thought the culprit was LCx with involvement of both lateral and posterior wall (STD appear to me maximal in V3-V4). The ST elevation in aVL with reciprocal STD in inferior leads and down-to-up T wave made me think about OMI rapidly but I cannot correlate the diffuse anterior STD depression apart from posterior wall involvement.
ReplyDeleteI agree, I would have thought LCx. However, an incomplete occlusion of the Diagonal artery probably caused ST subepicardial (transmural) (ST elevation in I, aVL) ischemia in its more distal distribution, and subendocardial ischemia (STD in precordial leads) in the more proximal distribution.
Delete