
A 51 yo male smoker with no other CV risk factors and no previous heart disease presented to a hospital without PCI capability complaining of 1.5-2 hours of severe epigastric pain radiating to the shoulders. He was diaphoretic and agitated. He had been treated for "flu" manifesting as fever and sore throat for 5 days. He was afebrile. He had no pericardial friction rub.
Here is his initial ECG:
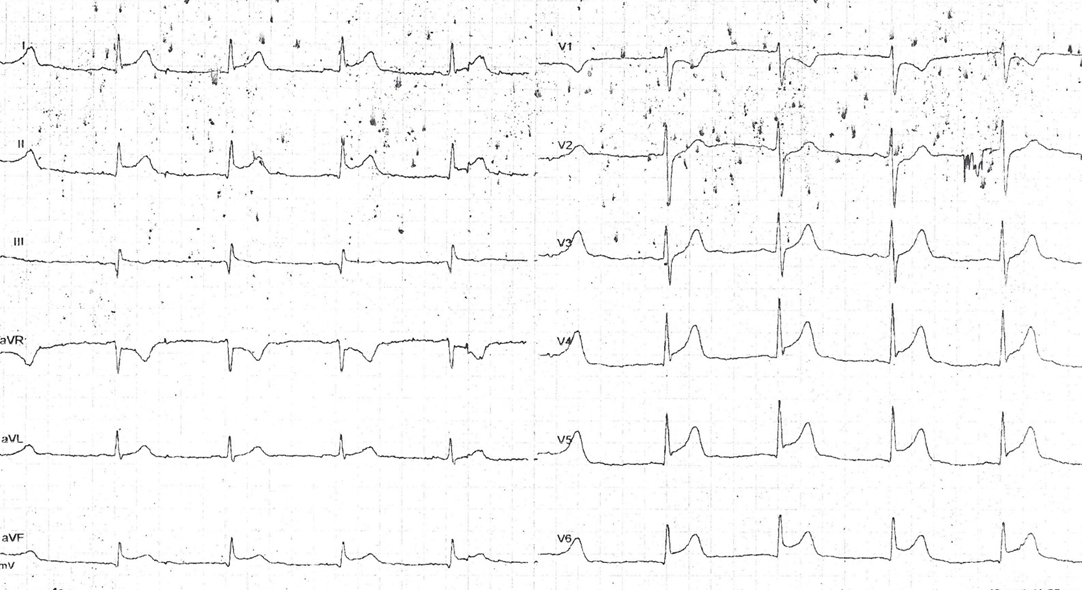 |
| There is sinus rhythm with a QTc of 434 ms. There is a possibly significant Q-wave in lead III. There is ST Elevation in leads I, II, aVF (+minimal in lead III) and V4-V6. The T-waves are not definitely hyperacute, but also possibly slightly enlarged. The ST vector is approximately 30 degrees, between leads I and II, opposite aVR, which has the most ST deviation (in this case, ST depression). And it is towards V5. There is no reciprocal ST depression in lead aVL (if there were, the ST vector would have to be greater than 60 degrees). There is no definitely excessive PR depression. There is ST depression in V1 also. Is there ST depression in lead V2? There is some artifact and wandering baseline. If there is ST depression in V2, it is very important. There is no appreciable PR depression. |
The obvious differential diagnosis here is inferolateral +/- posterior STEMI vs. Myo- or pericarditis (or baseline ST elevation -- early repolarization).
Favoring STEMI:
ST depression in V1 and possibly V2. One should never be confident in an ECG diagnosis of (myo-) peri-carditis if there is ANY ST depression. There may be ST depression in localized (as opposed to the much more common diffuse) pericarditis, but this is relatively rare.
Favoring Myopericarditis:
Absence of reciprocal ST depression in lead aVL. (In our study of 150 patients with inferior STEMI, 33 had ST elevation in leads V5 and V6 (inferolateral STEMI). All of them had some ST depression in lead aVL).
This is a very difficult ECG. I always say that "you diagnose pericarditis at your peril" because, if there is no rub or effusion, and the ECG is not absolutely typical of pericarditis, and the clinical scenario is consistent with STEMI, then you must act as if it is a STEMI.
The best way to rapidly differentiate is to do a high quality echocardiogram or, of course, just go to the cath lab.
Clinical Course
Clinical Course
A stat echo showed no pericardial effusion, but technique was inadequate to find or exclude a wall motion abnormality.
The initial troponin I returned at 8 ng/mL. (myopericarditis? or STEMI?)
With suspicion of STEMI, the patient was promptly transferred to a PCI-capable hospital
(door-to-door time: 30 minutes) and had this ECG on arrival:
 |
| Now there is much less ST deviation. This would be rapid evolution for myopericarditis, and more typical of a coronary thrombus (or spasm) that has lysed (resolved). |
He underwent coronary angiography by a very experience angiographer which ruled out coronary occlusion and had normal coronary arteries. However, there was no IVUS (intravascular ultrasound) to absolutely prove absence of extralumenal plaque with culprit).
After angiography the patient was taken back to the hospital where he first presented
and was treated as for myo-pericarditis with anti-inflammatories. A repeat high quality echocardiogram showed minimal pericardial effusion in the posterior and lateral sides. There was no evidence of wall motion abnormality.
After angiography, troponin I peaked at 18.120 ng/ml with a rapid fall thereafter to 0.143 ng/ml on day 4.
Here is the ECG on day 2:
 | ||
| All ST deviation is resolved. There is T-wave inversion in I and aVL. This evolution is consistent with either myopericarditis or STEMI |
And here is the ECG on day 3 (48 hours):
 |
| Unchanged |
No MRI or biopsy was done to prove or disprove myocarditis. There was a mildly elevated CRP and ESR.
Troponin: Does a rapid rise and fall of troponin indicate STEMI with reperfusion rather than myocarditis? One would think so, but I have not been able to find any hard data on this. I have seen many cases of purported, but not proven, myocarditis that had a rapid rise and fall. As inflammation is a more constant process than ischemia and reperfusion, I would have guessed that it would have a more steady elevation of biomarkers. Does anyone know? The "state of knowledge" paper referenced above makes no comment on this.
In this study of 625 patients with presumed STEMI who had angiograms within 2 hours of the ECG, but not simultaneous with the ECG, 26 had completely normal angiograms. The final clinical diagnosis by 3 cardiologists (not by MRI or biopsy) was STEMI in 7 (1.2%) and myopericarditis in 5 (0.8%). Normal angiograms (no stenosis at all) seem to occur in about 4.5% of patients with Non-STE-ACS, but they still have substantial subsequent morbidity (2% death or MI at 1 year; TIMI score stratifies them well)
Finally, there is this paper by Sarda et al. from JACC in which they studied 45 patients with apparent STEMI but with normal coronary arteries. They used Indium scintigraphy to assess whether it was MI or myocarditis. In 35 of 37 cases with adequate followup, it was myocarditis. In 2, it was MI. However, this article states that scintigraphy has poor sensitivity and specificity for myocarditis: "Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases."
Was the initial management correct? Yes. This could have been STEMI and should be managed as such. It still might have been STEMI. The ST depression in V1 and V2 is particularly worrisome. Had it been possible to get a high quality echocardiogram at the time of the ST elevation, and it had been completely normal, then it would have been reasonable to diagnose myopericarditis without an angiogram.
What is the diagnosis? Is it clearly and unequivocally myocarditis? The diagnosis can't be made for certain without MRI, biopsy or at least a pericardial friction rub. There was an effusion later on echo, strongly supporting the diagnosis. Additionally, profound PR depression (or elevation in aVR) would be very supportive.
Great case and summary. I've currently got maybe a half-dozen pericarditis/myocarditis vs. STEMI cases saved up and waiting for follow-up (I tend to do them in batches), but a few feature surprisingly dynamic ST/T-wave changes. Do you have any information on just how rapidly we should be seeing the progression from ST-elevation to T-wave inversions and if there is a meaningful difference compared to true ACS? Like your thoughts on troponin, I would think the ECG would also be less rapidly evolving in myocarditis but I really have no good info on that. Thanks for the case and discussion.
ReplyDeleteVince, as far as I know there is no good data on this.
DeleteGreat case,
ReplyDeleteinstructive and sobering
I always follow your clinical cases with interest.
Thank you Dr. Smith.
Vittorio
I agree with Vittorio. I go on different EKG Blogs to read and learn often. Yours is definitely the most interesting. Let me know if We can help with anything.
ReplyDeletehttp://cardiologyforless.com/EKG-Machine/
Great case good follow up sir
ReplyDelete