A 60 yo female presented by ambulance in resp distress, requiring noninvasive ventilatory support. She had pulmonary edema and was near respiratory failure.
Here is the prehospital ECG (will not comment on the interpretation until the end of the post, so you can ponder it for yourself):
 |
| Computer read: "Sinus tachycardia" at a rate of 143, and "***Acute MI***". Obviously, there is no clear STEMI. |
She was continued on respiratory support, treated for COPD and CHF with nebs, steroids, lasix and nitro. Here is her first ED ECG:
 |
| The computer reads "sinus tach". |
An ED bedside echo was performed from the subcostal view:
 |
Here is a legend for what you are seeing on the echocardiogram: LA = Left atrium, LV = left ventricle, RA = right atrium, RV = right ventricle, MV = mitral valve. The LA is greatly enlarged. The LV is very small. The mitral valve is very echogenic and highly suggests stenosis, which we confirmed with doppler.
|
Chart review confirmed h/o porcine mitral valve replacement with subsequent development of prosthetic mitral valve stenosis (that is to say, it recurred in the new valve). This conforms with our ED echo.
The heart rate continued at 143, and by this time there was much less artifact. This strip was printed out:
 |
| Now there is clear atrial flutter. |
A bit of history could be obtained at this point, and she said she had had rather sudden SOB about 15 hours prior, and had had some pink and frothy sputum.
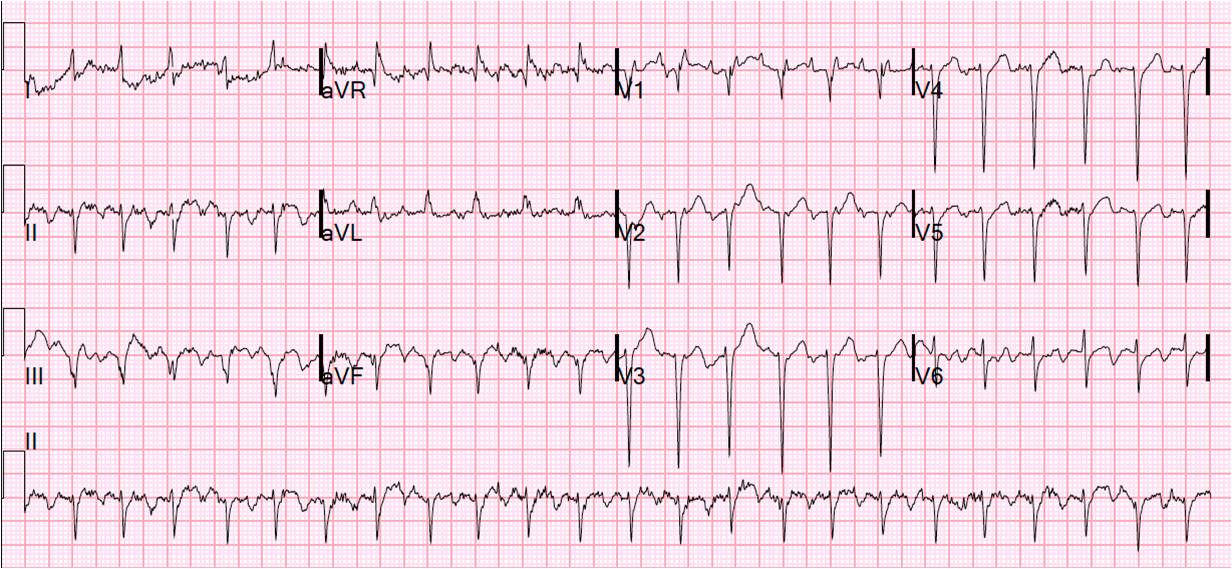
A better 12-lead was obtained:
 |
| Now, again, the atrial flutter is obvious, and there are no signs of ischemia |
So, we have a patient who is in respiratory distress, due to mitral stenosis and complicated by atrial flutter, which diminishes LV filling that is already compromised by mitral stenosis. ACLS would say to do electrical cardioversion for a patient with atrial flutter and rapid ventricular response who is suffering respiratory failure, but patients with mitral stenosis are at very high risk of thromboembolism and stroke (old literature). Cardioversion would increase this risk. Therefore, we decided on slowing the ventricular rate with diltiazem. Here is the subsequent ECG:
 |
| There is now atrial flutter with 4:1 block. |
With more time to fill, the LV was able to pump better. The patient improved gradually, and refused a valve replacement. She returned a few days later in distress and will now get a new valve.
Look again at the first ED ECG:
|
| Knowing that it is atrial flutter, you can now see (if you didn't before) the atrial spikes in V1 (2:1) that might have been interpreted to be artifact. |
Learning points:
1) When the heart rate does not change, but stays rapid and constant, it is probably not sinus tachycardia and then you should...
2) Look for atrial flutter waves
3) ACLS is guidelines only. Sometimes the patient does better with less aggressive care (and, of course, sometimes with more). One must always think it through.
4) Bedside echo can be very useful






Dr. Smith,
ReplyDeleteI believe the patient also has a LAFB throughout the ECGs. Also on the first 12-lead the patient has a RV strain but would the non-invasive ventilatory support (CPAP?) change it?
V1 and V2 are oddly upright in the prehospital ECG but unequivocally not in the hospital ECGs. Do you think this is part of the pathological process or just lead placement problems?
ReplyDeleteAs for the first in-hospital ECG, a pseudo-R' in V1 caught my eye. Interesting morphology of the flutter waves!
Troy, you're right about the LAFB. I didn't comment much on anything except the rhythm and the lack of ischemia, and, to be complete, I should have. There is left axis, probably LAFB. On the true first ECG (prehospital), there are tall R-waves in V1 and V2 which must be artifactual, but I'm not sure how they got that way. On the others, there is poor R-wave progression consistent with her COPD.
ReplyDeleteThanks for pointing that out.
Steve Smith
Yes, exactly! V1 and V2 must be artifact.
ReplyDeleteDr. Smith,
ReplyDeleteI love the new format. Just wanted to let you know that I learn a lot from your blog and appreciate what you are doing.
Thanks a lot.
Javier,
ReplyDeleteI appreciate the feedback!
Steve Smith
Dr Smith do you have your own style in differentiating VT vs SVT? I have seen many algorithms including Brugada and Vereckei, but I'm very interested if you have your own style?
ReplyDeleteThanks. Sorry for the completely irrelevant question from the blog post.
I've been meaning to post on this for a long time, and will. But, in the meantime, I first look for several things:
ReplyDelete1) look for hidden p-waves before each QRS! don't miss sinus
2) If there is a transition from narrow to wide, is the rate the same? then it must be SVT.
3) Does it immediately look to me like RBBB or LBBB? Then it is SVT
4) quick look for obvious fusion beats and AV dissociation. If found, then VT
5) quick look for concordance (all QRS's in the same direction in precordial leads, not the same as concordance when evaluating ST segments in LBBB)
6) QRS duration: VT should be > 140 ms (except for fascicular VT), and the longer the more likely to be VT
7) Finally, I like a new rule better than Brugada or Vereckei #1 or Vereckei #2 (aVR). It is Sasaki's rule:
Step 1: Initial R in aVR?
If yes, then rhythm is VT. If no, step 2.
Step 2: Interval from onset of R wave to the nadir of the S ≥ 100 msec (0.10 sec) in any precordial leads?
If yes, then rhythm is VT. If no, step 3.
Step 3: Initial r or q ≥ 40 ms in any lead?
If yes, then it is VT.
If no, then it is SVT
Sasaki K. Circulation 2009; 120:S671