
Sent by anonymous, written by Pendell Meyers
A woman in her 40s with no known comorbidities presented with acute chest pain radiating to left arm and neck, which started approximately 4 hours prior to arrival. Vitals were reported as within normal limits except for tachycardia.
Here is her first ECG on arrival:
 |
| Original image. |
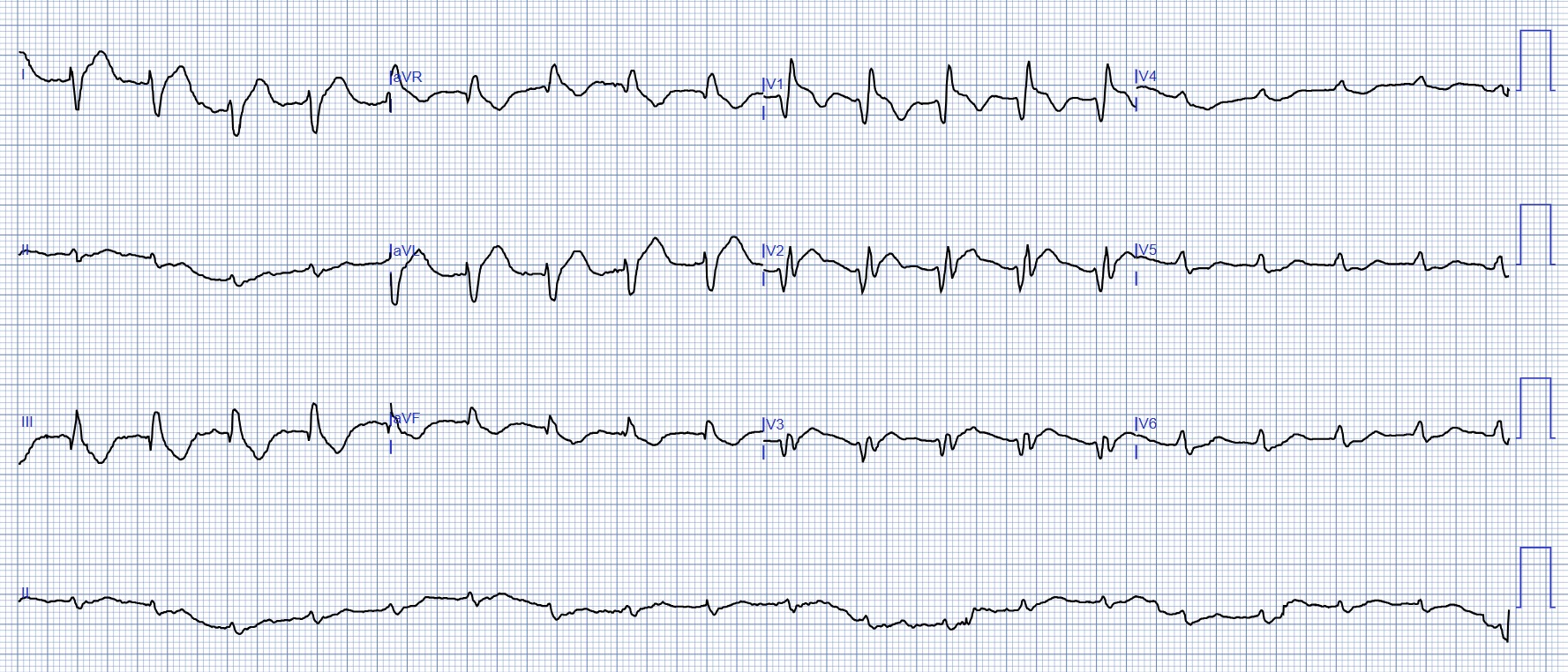 |
| PMcardio digitized image. What do you think? |
Anyone who has been a reader of this blog understands the terrible significance of this ECG, which is diagnostic of acute proximal LAD occlusion. There is RBBB and concordant STE in V1-V3, as well as reciprocal STD in V5-6 ("precordial swirl"), as well as hyperacute T waves in I and aVL, with reciprocally negative HATWs in III and aVF. Anterolateral OMI, likely with acutely ischemic RBBB, all due to proximal LAD OMI.
Side note: I think the rhythm is probably sinus tachycardia, but I can't easily point out the sinus P waves. (See Ken Grauer comment below for further rhythm interpretation on this one!).
Side note: I think the rhythm is probably sinus tachycardia, but I can't easily point out the sinus P waves. (See Ken Grauer comment below for further rhythm interpretation on this one!).
________
Also:
Lead Reversal!
Jose Alencar noticed something here: there is Right Arm/Right Leg lead reversal. This reversal causes lead II to be flat (almost or completely isoelectric), and causes lead I to resemble aVL and lead aVF to resemble aVR.
Without this reversal, the QRS would be mostly negative in inferior leads and upright in aVL.
I (Smith) expected to see Left Anterior Fascicular Block (LAFB) but did not, and this lead reversal, which I had not noticed, explains why not. (For more on this lead reversal — See KG Comment in the Addendum below).

________________
Here is the Queen of Hearts interpretation, appropriately reading STEMI equivalent, highlighting anterior and lateral leads with explainability, and even detecting reduced LVEF. Anyone who has seen and studied OMI patients knows that this patient with proximal LAD pattern, with super high risk ischemic RBBB, and tachycardia, is in cardiogenic shock until proven otherwise. This pattern has very high mortality.

The Emergency Physician contacted the Cardiologist immediately asking for cath lab activation.
The Cardiologist stated that the ECG did not show signs of STEMI, but rather NSTEMI, recommended serial ECGs and troponins, and cancelled the activation request.
Approximately 15 minutes later, a repeat ECG was performed:
 |
| Original image. |
 |
| PMcardio digitization. |
Very lucky for the patient, there is a brief period with a functional Right Bundle Branch (RBB), allowing the Cardiologist to see the same situation without the complication of the RBBB. Without the RBBB, I think most everyone would call this "STEMI." Lucky for the patient, the Cardiologist now agreed that she was having a "STEMI" and agreed to do the angiogram.
The angiogram showed ostial 100% LAD thrombotic occlusion which was opened.
Echo later that day showed an EF of 35%, with dense anterior and apical wall motion abnormality.
Troponins were rising rapidly but not measured to peak.
She survived the hospitalization, but long term outcome is not available.
Discussion:
This patient was very lucky that she had a doctor who understood her initial ECG, advocated for her, performed serial ECGs, and that her serial ECGs happened to have temporary lack of RBBB which reduces the complexity of the ischemia interpretation. The result in this lucky case was only about a 15 minute delay. Many patients are not this lucky. I would prefer that all Emergency Physicians and Cardiologist learn this pattern and its significance, but this is just not the world that we live in currently, with the STEMI paradigm. I am encouraged by people like the one who sent me this case, and I hope that AI can soon help bridge this gap.
See some of our many related posts on this deadly pattern:
One of those ECGs you need to instantly recognize, which learners may struggle with at first
Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin.
An elderly woman with acute vomiting, presyncope, and hypotension, and a wide QRS complex
A man in his 40s who really needs you to understand his ECG
Cardiac Arrest at the airport, with an easy but important ECG for everyone to recognize
===================================
Please NOTE — I am adding this Addendum after I wrote My Comment that appears below. I still wonder about the rhythm in the initial ECG in today's case — which could even be sinus rhythm (as Dr. Meyers suspected) — but which we unfortunately have no way of knowing as to what lead II would have shown if limb leads had been correctly placed.
===================================
ADDENDUM (April 16, 2024):
I love lead reversals — and together with my colleague contributors to Dr. Smith's ECG Blog, we have pointed out many of these "technical misadventures" among the cases sent to us (See the LIST at the end of My Comment in the January 6, 2024 post in Dr. Smith's ECG Blog).
- The above said — I missed the RA-RL reversal in today's post!
- Medicine is humbling. Just when we think we have "mastered" a clinical entity — we are "brought back to earth" with something we missed. BEST approach is to learn from this.
Why I missed today's lead reversal:
- I knew that the presence of a flat line in any of the standard leads (I,II,III) — is immediate indication of some type of lead reversal (See My Comment in the October 12, 2024 post). But until now — I did not appreciate that an almost flat line (as in today's post) indicated the same. I now know better.
- As always — my favorite on-line "Quick GO-TO" reference for the most common types of lead reversal comes from LITFL ( = Life-In-The-Fast-Lane). I have used the superb web page they post in their web site on this subject for years. It’s EASY to find — Simply put in, “LITFL Lead Reversal” in the Search bar — and the link comes up instantly.
- Below in Figure-A — is the summary from this LITFL page as to what happens with RA-RL reversal. Unfortunately — there is no way that I know with RA-RL reversal to figure out what today's initial ECG would have shown, had the limb leads been correctly positioned.
- Probably — We would have seen LAHB (Left Anterior HemiBlock) — just as Jose Alencar suspected! This of course makes perfect sense given the "Swirl" pattern from acute proximal LAD occlusion in today's case (ie, RBBB/LAHB is a very common complication of acute proximal LAD OMI! ).
- Possibly — We might have seen sinus P waves. Possibly not. If ECG #1 was sinus tachycardia — I still would have expected to see P waves in some other leads. But unfortunately, we will never know the answer to this — and my point in My Comment below still holds — that we need to always look first at lead II to see if there is or is not an upright P wave.
- Learning Points for Me: An almost flat line in any standard lead may indicate lead reversal. Especially in the presence of an almost flat line — the absence of P waves in lead II (and in all other leads) should prompt us to look again for one of the possible types of lead reversal. Our appreciation to Jose Alencar for his "eagle eye"!
.png) |
| Figure-A: The effects of RA-RL Reversal (as per LITFL — and exactly as pointed out by Jose Alencar and Dr. Smith above). |
============================
NOTE: (April 16, 2024):
— What appears below is what I wrote before today (and before I wrote the above Addendum).
============================
===================================
MY Comment, by KEN GRAUER, MD (4/15/2025):
===================================
I was intrigued by the 2 ECGs in today's case.
- For clarity in Figure-1 — I've reproduced the PMcardio versions of these 2 tracings. To facilitate comparison — I've placed both tracings together in this figure.
- This diagnosis should not have been missed by the Cardiologist on call.
- Fortunately, the ECG was repeated just 15 minutes later (by an astute ED physician) — and the 2nd tracing was correctly identified by the Cardiologist as an acute STEMI, in need of prompt cath.
- Along the way — I believe the initial cardiac rhythm (in ECG #1) was overlooked.
- To Emphasize: Regardless of what the initial cardiac rhythm was — this patient with new CP is in process of evolving an acute LAD OMI that needs prompt reperfusion with PCI (which would probably have fixed the initial rhythm had it persisted). That said — my goal is to offer an additional perspective on some of the more subtle-but-important points manifested by these 2 tracings.
- Warning: What follows is a "deep dive" into the cardiac rhythm of ECG #1. My hope for those who stay with me, is to convey the simple wisdom as to how adding a targeted 5 seconds to your ECG interpretation routine can prevent the rhythm oversight illustrated by today's case.
Is the Initial Rhythm Sinus?
By definition — a sinus mechanism is present in a regular rhythm when the P wave is upright in lead II. This is because spread of the depolarization wavefront, as it moves from the SA Node to the AV Node — is oriented in a direction close to +60 degrees in the frontal plane (with +60 degrees corresponding to the electrical axis location of lead II ).
- If the P wave is not upright in lead II — then you do not have sinus rhythm.
- There are only 2 exceptions to this rule: i) If there is dextrocardia; or, ii) If there is lead reversal.
- While true that on occasion, the P wave with sinus rhythm may be of very low amplitude — there should be a P wave.
The rhythm in ECG #2 is clearly sinus (at a rate of ~95-100/minute) — since a distinct, upright P wave with constant PR interval is consistently seen (RED arrow in lead II). Smaller P waves of different morphology are seen in other leads (PINK arrows).
- In contrast — No P waves at all are seen in ECG #1. WHITE arrows highlight where we would expect to see sinus P waves if they were present (Note that there is no sign of any P wave in any of the 19 beats in the long lead II rhythm strip).
- Of note — If anything, the PR interval shortens with tachycardia. As a result — IF sinus P waves were present in ECG #1 — they would not be hidden within the preceding ST segment unless there was a very long 1st-degree block (which is highly unlikely given the definite sinus rhythm with normal PR interval in ECG #2 that was recorded just 15 minutes later). Therefore — the rhythm in ECG #1 is not sinus.
What then is the Rhythm in ECG #1?
In short — I don't know.
- What we do know — is that the rhythm in ECG #1 is regular at a rate of ~115/minute — with a wide QRS (that manifests an RBBB conduction pattern) — but without any sign of atrial activity.
- Regularity of the rhythm rules out AFib.
- Especially given the marked right axis (rS pattern in lead I with predominant negativity) — I considered fascicular VT.
- Narrow initial deflections of the QRS in many leads suggested it more likely that the rhythm was arising from somewhere within the conduction system (ie, junctional tachycardia?; an accelerated His rhythm?).
- Especially given resolution of the RBBB conduction pattern 15 minutes later, at which time heart rate had slowed from ~115/minute to the rate of 95-100/minute seen in ECG #2 — rate-related aberrant conduction of a supraventricular rhythm seemed a good bet. That said — the tiny isoelectric QRS in lead II of ECG #1, and the highly unusual 4-phasic rSR's' morphology in lead V2 are atypical for aberrant conduction.
- Bottom Line: I was not sure of the rhythm diagnosis in ECG #1. My hunch was junctional tachycardia with rate-related aberrant conduction — but regardless of what the rhythm in ECG #1 was, as long as the patient remained hemodynamically stable — prompt cath with PCI was the treatment of choice for both the acute MI as well as the tachycardia.
- Is there an upright P wave with constant PR interval in front of each QRS complex in the long lead II rhythm strip? If not — then the rhythm is not sinus (assuming no lead reversal or dextrocardia).
- With minimal practice — all it takes is 3-to-5 seconds to quickly scan the long lead II. After you do so — you can then turn your attention to the 12-lead.
-USE-USE.png) |
| Figure-1: Comparison between the 2 ECGs in today's case. (To improve visualization — the original ECGs have been digitized using PMcardio). |
We owe credit for the term "Precordial Swirl" to Drs. Meyers and Smith (See the October 15, 2022 post in Dr. Smith's ECG Blog). This insightful designation facilitates recognition of a very proximal site of LAD occlusion (usually proximal to the 1st septal perforator) — with resultant septal ischemia in addition to anterior wall and apical involvement.
- Regardless of what the rhythm in ECG #1 turns out to be — the diagnosis of "Swirl" is secure because there is anterior lead ST elevation that begins in lead V1, with ST segment flattening and depression in lateral chest leads V5,V6.
- With both RBBB conduction and fascicular VT — the abnormal ST segment shape and ST elevation that is clearly present in leads V1,V2,V3 of ECG #1 simply should not be there. (Keep in mind that normally with RBBB conduction — anterior chest leads should show ST-T wave depression and not the elevation that we see here! ).
- The deep and wide Q waves in leads V1 and V3 (and almost in lead V2) — suggest there has already been significant injury.
Final Curiosity:
Did you notice the bizarre short pause that occurs at the very end of ECG #2?
- Whereas I initially thought the flat line at the end of the long lead II in ECG #2 was the result of some technical mishap (RED question mark) — the presence of what looks to be a P wave occurring just before the standardization marker (BLUE arrows in ECG #2) made me question this initial impression — especially given the acute evolving extensive anteroseptal infarction that minutes earlier in ECG #1 manifested RBBB conduction with marked right axis.
- Bottom Line: While I still suspect this short pause at the end of ECG #2 is the result of some technical mishap — given the clinical situation of extensive anteroseptal MI in progress, close observation of the rhythm to ensure this is not the onset of a Mobitz II block would seem to be in order.






-USE.png)
-USE.png)