A 50 yo was resuscitated from ventricular fibrillation.
He had a prehospital ECG recorded after ROSC:

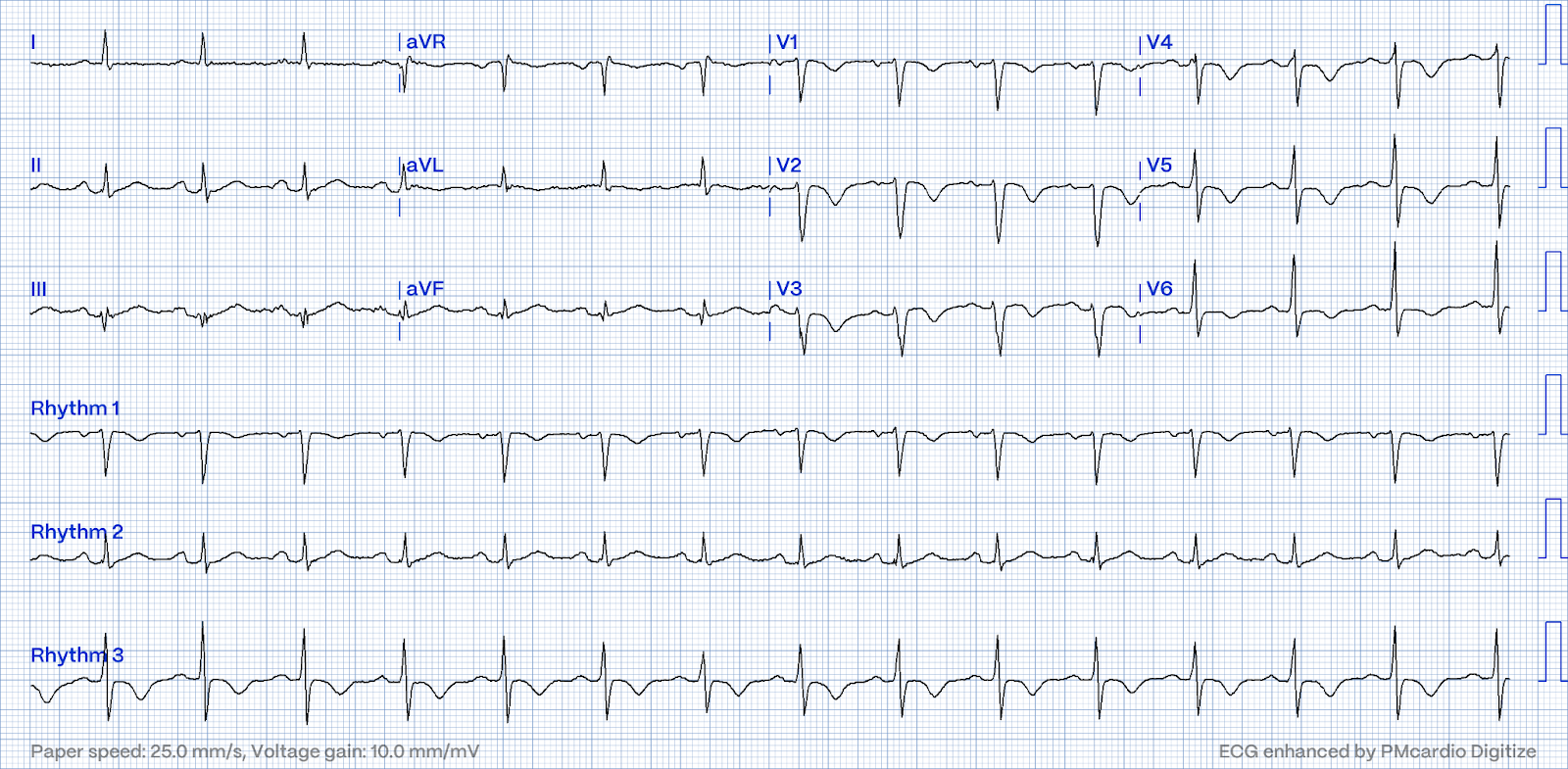
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. Although one may have all kinds of ischemic findings as a result of cardiac arrest (rather than cause of cardiac arrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion.
This prompted cath lab activation.
On arrival to the ED, this ECG was recorded:

There is profound ST depression maximal in V1-V4. This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. But without seeing that first prehospital ECG, I would call this: "Posterior OMI until proven otherwise."
Of course the Queen of Hearts also sees OMI:

Click here to sign up for Queen of Hearts Access
Another ECG was recorded 13 minutes later, well after ROSC and with more stable vital signs:

This is diagnostic of posterior OMI.
Of course the Queen of Hearts sees OMI on this one as well:

Click here to sign up for Queen of Hearts Access
Posterior leads were recorded. It was unusual that the leads that were shifted around to the back, as V7-V8, were V1-3 (usually one puts V4-6 on the back)

How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
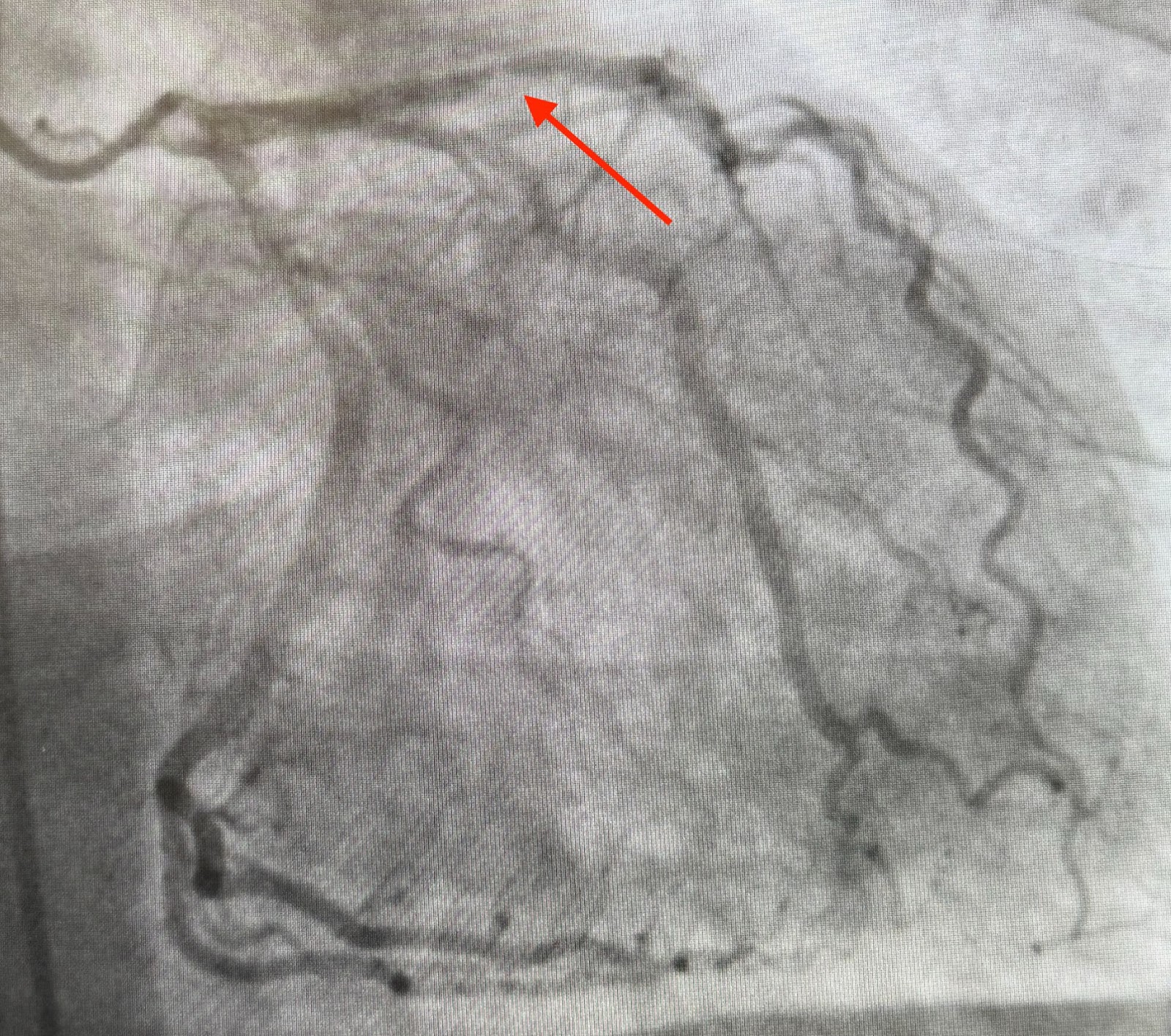
The angiogram explains it:
Culprit for OOHCA/VF is an acutely occluded mid-Circumflex Patient is incidentally noted to have chronic occlusion of the mid LAD with robust R > L collaterals.
In other words, the LAD distribution is supplied by the RCA.
LMCA:
Left main is a large caliber vessel
LCx: Circumflex is a medium-large caliber vessel that is occluded in the mid-segment on initial angiography. TIMI-0 flow.
On follow up angiography, there was a large OM1 and small AV groove Cx/LPL
visible as the vessel re-canalized
LAD is noted to have diffuse 50% stenosis in the proximal segment and is
occluded immediately beyond a small D1
RCA is a medium-large caliber vessel and supplies a medium rPDA, medium rPLA1, and three small rPLA branches.
There are well developed R > L septal collaterals that fill a majority of the mid and distal LAD
Explanation:
The acute circumflex occlusion caused the arrest. The arrest caused extreme hypotension which rendered the RCA incapable of continuing to supply the distant LAD. This caused a type 2 anterior STEMI.
In other words, with a chronic total occlusion of the LAD and collaterals from the RCA, the collaterals were not sufficient to supply the LAD distribution while the patient was in arrest.
Peak troponin I > 60,000 ng/L
Formal Echo
Normal left ventricular cavity size, mildly increased wall thickness, and moderately to severely reduced LV systolic function. The estimated left ventricular ejection fraction is 29%.
---Regional wall motion abnormality--entire apex dyskinetic, mid anteroseptum, mid anterior wall akinetic.
---Regional wall motion abnormality--anterolateral akinesis.
---Regional wall motion abnormality--mid and distal inferolateral wall
akinesis.
In other words: 1) infarct of the LAD territory (much of which could be old) and 2) inferior-posterior-lateral infarct.
MY Comment, by KEN GRAUER, MD (9/29/2024):
- Today's case reminds us of the intuitive logic that if a patient has a shockable arrest (ie, VFib) — and following successful defibrillation shows evidence of acute OMI (even if STEMI criteria are not necessarily fulfilled) — that such patients have much to gain from immediate cath with PCI. (See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog).
- Although predicting the "culprit" artery of acute coronary occlusion is often straightforward (ie, based on the distribution of leads with ST elevation and leads with reciprocal ST depression) — this is not always the case.
- The LIST of reasons why prediction of the "culprit" artery may not be straightforward include: i) Anatomic variants; ii) Multivessel disease; iii) Unusual patterns of collateralization (which are usually associated with multivessel disease); and, iv) The diagnosis may be wrong (ie, the patient may have Takotsubo cardiomyopathy — SCAD [Spontaneous Coronary Artery Dissection] — coronary artery spasm — acute pulmonary embolism — or something else).
- Relevance to Today's CASE: As per Dr. Smith — Trying to predict the "culprit" artery in today's case was confusing. The dramatically changing distribution of ST-T wave elevation and depression first predicted one — and then soon after, another "culprit" vessel. Learning from the results of cardiac catheterization that 2 of the reasons in my above LIST [multivessel disease and unusual collaterization pattern] account for this difficulty — helps us to understand the ECG findings in today's tracing.
- I believe trying to predict the culprit artery improves our ability at ECG interpretation — because it forces us to correlate ECG findings in all 12 leads with the clinical situation. For example, once we're able to appreciate if the ECG(s) in front of us does or does not clearly suggest a specific "culprit" artery — we know whether to contemplate one of the 4 reasons I cite in my above LIST.
- The September 9, 2024 post by Dr. Frick illustrates how trying to predict the "culprit" artery helped the interventionist — because knowing that the initial ECG strongly suggested Precordial "Swirl" (therefore diagnostic of a proximal LAD OMI) — meant that despite only minimal intraluminal narrowing of the LAD on cath, IVUS (IntraVascular UltraSound) would be needed for definitive diagnosis (and IVUS confirmed the culprit location suggested from the initial ECG).
- The April 8, 2022 post by Drs. Fetterolf and Meyers illustrates how recognizing the South African Flag Sign, in which there is ST elevation in only 1 chest lead ( = lead V2) — strongly suggested that despite lack of STEMI criteria (that require sufficient ST elevation in 2 consecutive leads) — OMI from acute occlusion of either the 1st or 2nd Diagonal Branch of the LAD was almost certain to be present.
- The September 23, 2024 post by Dr. Frick showed RBBB with ST elevation in leads V1 and V2 that might easily suggest either proximal LAD occlusion or proximal RCA OMI with acute RV involvement. But because Dr. Frick's assessment of the remaining 10 leads on this tracing was not consistent with OMI from acute occlusion of any specific coronary artery — consideration was given to an alternative diagnosis. Prompt identification of acute PE may not have happened if the clinician had not followed through the thought process in searching for a specific "culprit" artery.
- Especially important for emergency providers — our presentation to a doubting interventionist becomes more convincing, when despite being passed off as a "NSTEMI" — we are able to predict what the catheterization that eventually gets done will show.






-labeled-USE.png)
-USE.png)