
Written by Pendell Meyers
A young man in his 20s with history of end stage renal disease and dialysis presented for acute chest pain. His last dialysis was 4 days ago. He was very hypertensive and short of breath, but oxygen saturation was normal.
 |
| What do you think? |
Prior ECG on file from 12 days ago:
 |
| Baseline LVH with repolarization abnormalities. |
 |
| What is the rhythm here? |
 |
| Dramatic improvement, with QRS narrowing and reorganization of rhythm. |

===================================
MY Comment by KEN GRAUER, MD (10/21/2020):
===================================
As we have emphasized on numerous posts in Dr. Smith’s ECG Blog — Hyperkalemia must be recognized promptly! If it isn’t — the disorder may progress to life-threatening VT, as occurred in today’s case.
- The “good news” — is that rapidly-acting, highly effect treatment is available (as per the Calcium, Insulin & Dextrose, and Albuterol administered in today’s case that saved this patient).
NOTE: In the hope of supplementing the clinical points brought out in the above discussion by Dr. Meyers — I focus my comments below on a number of Advanced Points. My GOAL is to enhance appreciation and facilitate rapid recognition (and long-term care) of patients who develop life-threatening hyperkalemia.
- I have previously reviewed the “Textbook” Sequence of ECG Findings expected with progressive severity of Hyperkalemia (For Review — Please SEE My Comment that appears at the bottom of the page in the January 26, 2020 post of Dr. Smith’s ECG Blog).
Regarding today’s case — Dr. Meyers highlighted pathognomonic ECG features of life-threatening Hyperkalemia that were seen in the 1st tracing shown above. These included:
- QRS widening.
- Tall, peaked T waves.
- A rhythm disturbance ...
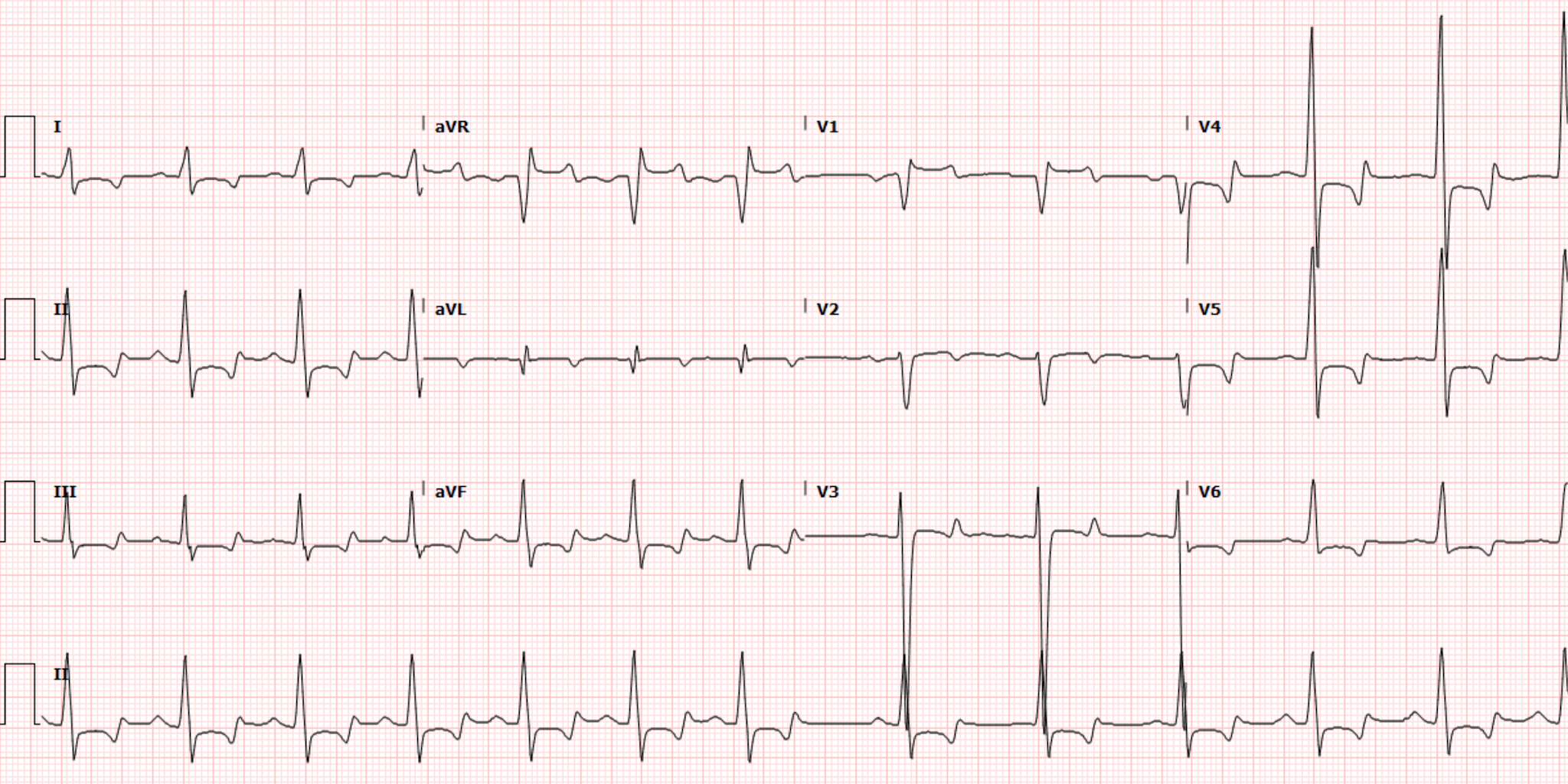
That said — there is MORE to discuss regarding the 1st tracing in today’s case. Please TAKE another LOOK at ECG #1 — which I’ve reproduced in Figure-1.
- In addition to QRS widening and peaked T waves — WHAT else do you see in ECG #1?
- What is the RHYTHM in this tracing?

MY Thoughts on ECG #1:
- Often overlooked when assessing an ECG for Hyperkalemia — is that T waves may be inverted. When this happens — these negative T waves also tend to be peaked, thus forming a mirror-image of the slender, symmetric positive T wave peaking familiar to us all. ECG #1 goes one step further in showing us a number of biphasic T waves — which feature both negative and positive peaked components to the T waves in leads V4, V5 and V6. Please recognize that these pointed negative T wave components in these lateral chest leads are an ECG finding consistent with marked hyperkalemia.
- QRS morphology with significant Hyperkalemia may be varied. One may see any form of bundle branch block or hemiblock — or — there may be a very unusual QRS morphology that does not resemble any known conduction defect. This latter possibility is what we see in Figure-1 — in which a number of features similar to sodium channel blockade are seen. These include marked QRS widening (I measure a QRS duration of ~0.20 second in lead V3!) — an indeterminate frontal plane axis (nearly isoelectric complexes in 5/6 limb leads) — a prominent terminal R’ in lead aVR — and — marked QTc prolongation.
- The marked QTc prolongation seen in ECG #1 raises the possibility of associated hypocalcemia (which often accompanies hyperkalemia in patients with renal failure). Information regarding the serum Ca++ level wasn’t available in today’s case.
WHAT is the Rhythm in ECG #1?
It is often extremely difficult to determine the rhythm in patients with marked hyperkalemia. I found this true in ECG #1. Some of the reasons why rhythm determination may be so difficult with marked hyperkalemia are listed in Figure-2.
- I did not think P waves were visible in ECG #1. Instead of P waves in leads V1 and V2 — I thought the small biphasic deflections in the middle of the R-R interval in these leads were T waves — because their timing corresponds to the peak of the tall T waves in simultaneously-recorded leads V3 and the long lead II. I suspected a sinoventricular rhythm.
- Given other signs in ECG #1 that suggested marked hyperkalemia — if P waves were present, I would have expected them to be of smaller amplitude than the mid-interval deflections we see in leads V1 and V2.
- I did not see an upright P wave in lead II. (If the slight slurring we see on the downslope of the T wave in lead II is from a hidden P wave — the amplitude of such a P wave would be larger than I would expect in a patient with marked hyperkalemia).
- THE ABOVE SAID — I fully acknowledge that I could be wrong about a lack of visible atrial activity in ECG #1 (for all of the reasons I state in Figure-2).

WHAT Can We Learn from the Prior ECG on this Patient?
There is a lot we can learn about Hyperkalemia in today’s case from retrospective review of ECG #1 — in comparison to ECG #2, which is a prior ECG obtained on this patient 12 days before ECG #1 (Figure-3).
- Awareness of a brief History on today’s patient is invaluable for optimal clinical interpretation of the ECGs in this case: We are told that the patient is a young man in his 20s with end-stage renal disease, whose last dialysis treatment was 4 days ago. This patient presented with acute chest pain and dyspnea (with a normal O2 saturation) — with marked hypertension at the time he was seen.
- GIVEN this History — even before looking at ECG #1: i) Marked hyperkalemia may be anticipated, given that this patient is at least 1-2 days late for dialysis; ii) This patient is almost certain to have marked LVH — given end-stage renal disease and greatly elevated BP at the time he was seen; and, iii) It is likely that a non-cardiac cause of this patient’s acute chest pain will be found.
QUESTIONS:
- Do YOU think serum K+ was normal at the time this patient’s prior ECG ( = ECG #2) was done?
- WHAT other observations would you make from comparison of ECG #2 with ECG #1?

ANSWERS (My Thoughts on ECG #2):
We were not told what the serum K+ value was at the time ECG #2 was obtained — only that ECG #2 was a prior ECG obtained 12 days before ECG #1.
- Sinus rhythm at ~90/minute is present in ECG #2. Of note — the P wave is upright in lead II, and the P wave appears to be negative in lead V1. But P wave amplitude is small in leads V1 and V2 of ECG #2 — which supports my suspicion that those biphasic deflections in leads V1 and V2 of ECG #1 were too large to be P waves (especially since the initial serum K+ value = 9.3 mEq/L at the time ECG #1 was obtained — and P waves get smaller when K+ is markedly elevated).
- As expected — the prior ECG confirms marked LVH. For clarity regarding assessing the size of overlapping complexes in the chest leads of ECG #2 — I’ve colored in the S wave in lead V3 (which measures ~30 mm) and the R wave in lead V5 (which is ~31 mm) — which documents dramatically increased QRS amplitudes.
- Further supporting the ECG diagnosis of marked LVH in ECG #2 are: i) The History (the patient has end-stage renal disease with marked hypertension on admission); and, ii) That there are ST-T wave abnormalities in the lateral chest leads (ie, leads V5,V6) consistent with LV “Strain”. Taken together — these 2 factors dramatically increase specificity for true LV chamber enlargement.
- In addition to resolution of QRS widening — NOTE how different QRS morphology is between ECG #1 and ECG #2. Specifically: i) There is a marked difference in frontal plane axis between the 2 tracings (ie, The axis is indeterminate in ECG #1 — whereas the frontal plane axis was +45 degrees in the prior ECG); ii) The terminal R’ in lead aVR of ECG #1 was not seen in the prior ECG; and, iii) Amplitude of the QRS complex is very different in a number of leads (ie, LVH was not evident in ECG #1). BOTTOM Line: I found it interesting how dramatically (and how unpredictably) QRS morphology can change when serum K+ is extremely elevated.
WHAT do YOU Think Serum K+ was in ECG #2:
Review of this patient’s file provided us with a prior ECG on this patient obtained from 12 days earlier. But we are not told the circumstances under which ECG #2 was obtained — and we are not told the serum K+ level at that time. That said — I strongly suspect serum K+ was at least slightly elevated at the time ECG #2 was obtained! I say this because:
- Although modest in height — the T wave in lead V3 of ECG #2 is uncharacteristically pointed! This is not the normal appearance of an anterior lead T wave.
- The lowest point of the shallow inverted T waves in leads V5 and V6 is pointed. ST-T wave abnormalities due solely to LV “strain” do not do this.
- I would normally expect in a patient with marked LVH (to the extent that is obvious in ECG #2) — that there would be comparable ST-T wave changes of LV “strain” (ie, with a downsloping depressed ST segment — rather than the ST segment coving we see in leads V5 and V6 of ECG #2). I suspect the reason for this unexpected “strain” appearance in these lateral chest leads of ECG #2 — is that the downsloping ST depression that probably would have been seen if serum K+ was normal, has been attenuated by T wave changes from a serum K+ level that was at least slightly elevated at the time this prior ECG was done.
PEARL #1: Remember that the ST-T wave appearance seen on ECG in association with marked hyperkalemia is the net result of ST-T wave changes caused by increased serum K+ — superimposed on whatever the ST-T waves looked like before serum K+ became elevated!
- As a result — it is impossible to assess the ST-T wave changes for ischemia in ECG #1, because this tracing was obtained at a time when serum K+ = 9.3 mEq/L. In my experience — you never know what ST-T waves will look like until serum K+ is completely corrected and the ECG is repeated.
PEARL #2: The relevance of Pearl #1, is that even though the “textbook” sequence of ECG findings with increasing serum K+ levels is not strictly followed in all patients — in any given patient, the sequence for development of the ECG findings I illustrate in our January 26, 2020 post tends to be surprisingly consistent (in my experience) over the course of that patient’s hospital stay.
- I suspect the patient in today’s case is a frequent ED user. I say this because this young man has end-stage renal disease with dramatic LVH — he presented with life-threatening hyperkalemia (presumably the result of being late for his last dialysis treatment) — and, his prior ECG from just 12 days earlier also shows subtle-but-real signs of hyperkalemia at that time.
- I speak from my experience of reading all ECGs from 35 medical providers over a 30-year period, including frequent hospital Attending stints. As such — I got to know many of our clinic patients by their ECGs. As a result — I could sometimes immediately know for certain patients from their ECG (without need to first draw lab) if their serum K+ level was in the process of going up again.
- TAKE HOME Message — IF I was a medical provider charged with caring for today’s patient — awareness of what the serum K+ level was at the time ECG #2 was done would be insightful. Knowing this would help me with earlier recognition on return visits about when hyperkalemia was returning.

super case. super discussion. thank you, team.
ReplyDeleteThank you Tom! — :)
Delete