
Comment on ECG
Many immediately think this is pericarditis. But, in fact, this is the patient's baseline early repolarization, seen on a previous ECGs when he presented for a seizure (not chest pain). Most diffuse ST elevation is normal variant.
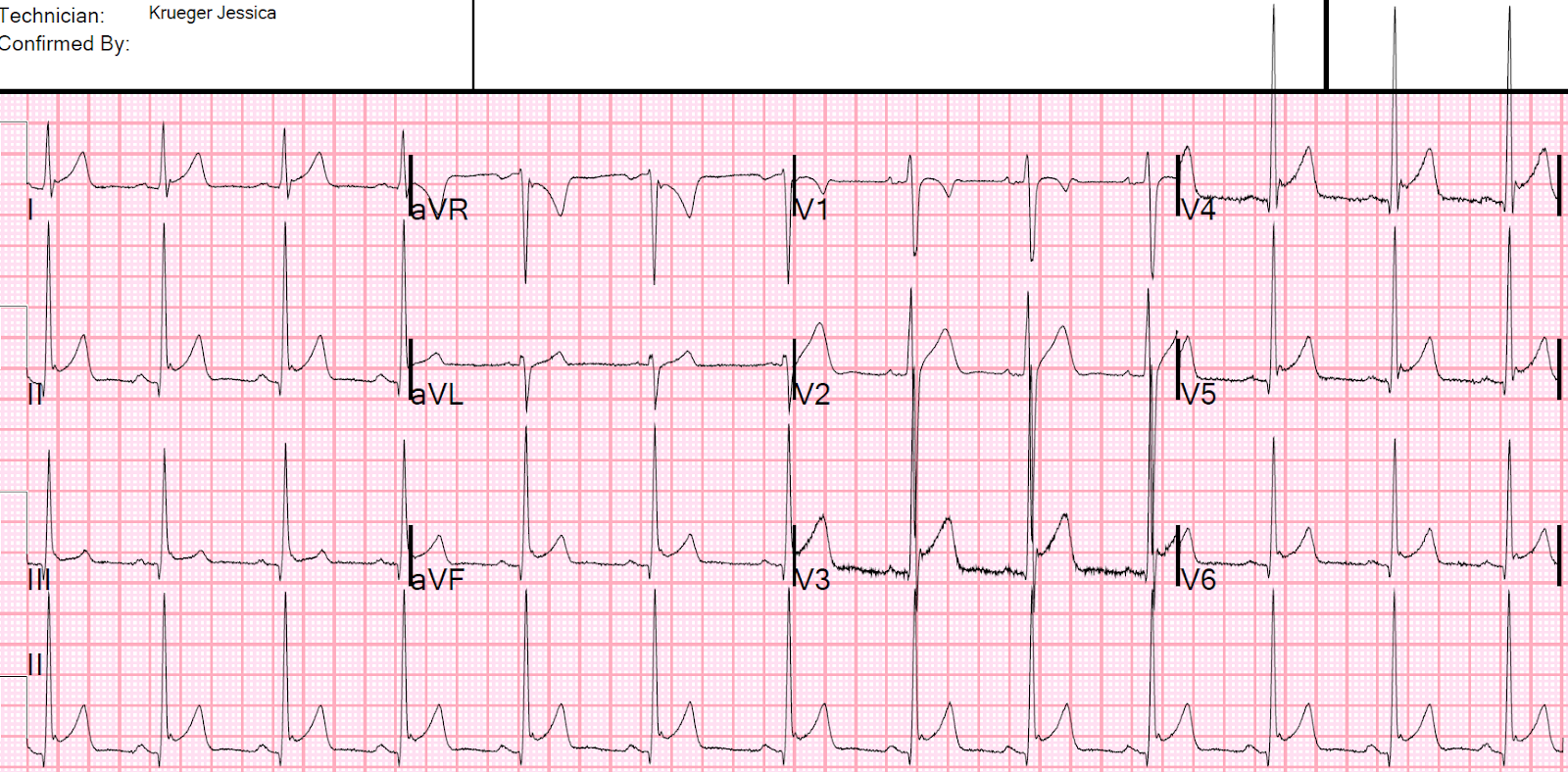
--There is diffuse ST Elevation.
--There are well-formed notches at the J-point in all leads with ST Elevation. The STE is called normal variant. The notching qualifies the ECG as true early repolarization (which is now defined as distinct from normal variant STE and does not even require any STE -- see reference below). Whether such notches also exists in pericarditis is uncertain; I suspect they exist in patients who have pericarditis superimposed on . We studied it in anterior MI vs. normal variant STE in V2-V4, and found that at least 1 notch of at least 0.5 mm in at least 1 of leads V2-V6 was found in 31% of normal variant and 14% of anterior MI.
--The only reciprocal ST depression is in aVR, but this is not significant (whenever there is diffuse STE, there MUST be STD in aVR since aVR is the (-) of a lead that would be between I and II. Other than aVR, we found that reciprocal ST depression is not found in pericarditis.
--There is minimal PR depression, though even some PR depression is normal; profound PR depression of at least 0.8 mm is reported as fairly specific to pericarditis, though the data is very sparse.
--There is some downsloping of the TP segment, which is known as Spodick's sign, which is reputed to be a good sign of pericarditis. Amal Mattu recently showed that Spodick's sign is not sensitive for pericarditis, and it has never been established (or even studied) as a means of differentiating pericarditis from normal variant early repolarization.
See Ken Grauer's additional comments below
Normal variant is FAR MORE COMMON than pericarditis.
General Comment
Nevertheless, in my experience physicians get some sort of delight in diagnosing pericarditis on the ECG. This delight causes bias.
Troponin was undetectable and patient had complete relief with an antacid.
Does it matter?
Yes. See this case that was written by Pendell Meyers when he was a medical student:
31 Year Old Male with RUQ Pain and a History of Pericarditis. Submitted by a Med Student, with Great Commentary on Bias!
In the case by Dr. Meyers, the providers assumed that because the patient had a previous diagnosis of pericarditis (made due to his ECG with diffuse STE), the diffuse STE again represented pericarditis. But in fact the patient NEVER had pericarditis and was suffering from pulmonary embolism which went undiagnosed because of this assumption.
The ECG diagnosis here is normal variant STE. It is ALSO true early repolarization.
True early repolarization is distinct from Normal variant ST elevation. It is defined in a 2015 consensus article in JACC as an end QRS notch of at least 1 mm, with or without ST Elevation.
True early repolarization is associated with a long term risk of ventricular fibrillation if found in middle-aged subjects. See this article in NEJM in 2009. See more reference for this in the above consensus article.

===================================
MY Comment by KEN GRAUER, MD (9/11/2020):
===================================
Dr. Smith texted me the tracing shown above for today’s case. He asked me the following questions:
- WHAT is the diagnosis?
- WHY do you say so?
The only clinical information I was given was, “Young man with chest pain.” I did not have the benefit of knowing there was a previous ECG.
- For clarity — I have reproduced ECG #1, and have labeled some findings to illustrate my impression (Figure-1):
 |
| Figure-1: Some findings on ECG #1 (See text). |
MY Interpretation of ECG #1: I thought this tracing was most suggestive of a repolarization variant. My systematic interpretation was as follows:
- The rhythm in ECG #1 is sinus with slight variation in rate — therefore sinus arrhythmia. All intervals (PR, QRS, QTc) are normal. The frontal plane axis is normal at +75 degrees, which makes for a fairly “vertical” QRS axis.
- Regarding chamber enlargement — there is no sign of LAA or RAA. QRS amplitude is clearly increased — with so much overlap of complexes in leads V2 and V3 as to make it difficult to count voltage. For clarity — I’ve colored the QRS complexes in these leads. The S wave in lead V2 measures 28 mm (RED S wave in V2) — and the R wave in lead V3 is 34 mm (BLUE R wave in V3). QRS amplitude is similarly increased in multiple other leads.
- PEARL #1: IF this patient was an older adult — then several of the voltage criteria for LVH that I’ve discussed in detail in My Comment to the June 20, 2020 post in Dr. Smith’s ECG blog would be easily satisfied. But QRS amplitude is often increased in younger adults (ie, under ~35 years of age) — which means that the specificity for LVH of the increased voltage that we see in ECG #1 is limited.
- PEARL #2: In addition to limiting specificity of voltage criteria for LVH — the other reason it’s important to appreciate how significantly increased QRS amplitude is in so many of the leads in ECG #1 — is that the relative amount of J-point ST elevation considered “normal” will be proportionately dependent on QRS amplitude in the lead being assessed.
Continuing interpretation by looking at Q-R-S-T Changes:
- Small and narrow Q waves are seen in infero-lateral leads (ie, in leads II,III,aVF; and V4,V5,V6). Given the fairly vertical frontal plane axis (+75 degrees) and the small size of these Q waves in comparison to the very tall R waves in each of these same leads — these are almost certain to be normal “septal” Q waves.
- R wave progression is normal — with transition (ie, where the R wave becomes taller than the S wave is deep) occurring normally between leads V2-to-V3.
Regarding ST-T Wave Changes:
- There is significant J-point ST elevation in multiple leads — that attains up to 3-4 mm in lead V3. The SHAPE of the elevated ST segments is concave-up (ie, “smiley” configuration — as per the small icon in RED in the right-upper corner of the tracing in lead V4).
- The T waves are inverted in leads aVR and V1 — but these are common normal findings.
- J-point notching is seen in multiple leads (GREEN arrows).
MY Impression of ECG #1: Reasons I thought the overall picture in ECG #1 was most likely to be a repolarization variant included the following:
- Although ACS (Acute Coronary Syndrome) can occur at any age — 18 years old is clearly a younger than is usually seen for ACS.
- Findings in ECG #1 that are highly characteristic of a repolarization variant include: i) The upward-concavity (ie, “smiley”-configuration) ST elevation shape that is seen in multiple (9/12) leads — without any localization; ii) Prominent J-point notching in multiple leads (GREEN arrows); iii) Markedly increased QRS amplitude — that proportionally minimizes the relative amount of ST elevation; and, iv) This tracing just “looks” like a repolarization variant. The main differential diagnostic considerations are acute MI and acute pericarditis — but ECG #1 does not look like either one of these.
Against ECG #1 being Acute MI:
- There is so much QRS amplitude, with prominent R wave voltage at an early point (by lead V2) in chest lead R wave progression.
- The QTc if anything looks fairly short.
- Q waves are small and narrow, and found in lead areas consistent with normal septal Q waves.
- ST elevation with acute MI usually localizes to 1 or 2 lead areas — but the ST elevation in ECG #1 is diffuse.
- There is no reciprocal ST depression.
- This tracing “looks like” a repolarization variant.
Against ECG #1 being Acute Pericarditis:
- As has been emphasized many times on Dr. Smith’s ECG Blog — acute pericarditis is far less common than acute MI or a repolarization variant among patients who present to an emergency setting. As per Dr. Smith, “You diagnose acute pericarditis at your peril!"
- There is no PR depression at all. While true that PR depression is neither very sensitive or specific as a sign for acute pericarditis — there is no PR depression at all here, and no more than trace PR elevation in aVR.
- The ST-T wave in lead II looks more like lead III than lead I. With acute pericarditis — the shape of the ST elevation in lead II tends to resemble the shape in lead I more than in lead III.
- There is prominent J-point notching in so many leads (GREEN arrows). While true that some J-point notching can be seen with acute pericarditis — it is rarely as marked as it is here.
- PEARL #3: The ST segment/T wave Ratio favors a repolarization variant — because the ratio is < 0.25 (See the magnified lead V6 insert in the bottom right portion of Figure-1). As I discussed and illustrated in My Comment on the December 13, 2019 post — the ST/T wave ratio is determined by comparing the vertical height of the ST elevation (from the end of the PR segment to the J point) in lead V6 — and comparing this to the amplitude of the T wave in V6. A ratio >0.25 suggests pericarditis — whereas <0.25 suggests a repolarization variant. As shown in Figure-1 — ST/T Ratio = 0.23, which supports my impression of a repolarization variant.
Philosophical Note = PEARL #4: I went back and thought a bit more about what Dr. Smith asked me = WHY does this tracing “look like” a repolarization variant, and not acute pericarditis to us? As I confessed in my “Editorial Note” in the December 13, 2019 post — I have generally not been an advocate of the ST/T Ratio, because of the difficulty in attaining consistency in measurements among practicing clinicians in an emergency situation.
- That said — I believe the rationale behind derivation of the ST/T Ratio is simple — namely, that in those uncommon situations in which acute pericarditis is truly present — there is usually a relative increase in the amount of ST elevation in lateral chest lead V6 compared to other leads with ST elevation. An ST/T Ratio >0.25 is one way to objectively quantify (based on data) this relative relationship. Another way (which with experience, my “eye” automatically does) — is to look at this tracing. Given the tremendous amount of QRS amplitude increase in so many leads on this tracing (witness the RED-BLUE color overlap in leads V2,V3) — my “eye” simply expected to see relatively more ST elevation in lead V6 if the patient had pericarditis. I then used the ST/T Ratio as an objective way to support my visual impression
BOTTOM Line: None of the above ECG findings I cite are perfect. There are always exceptions. That said — given the age of today’s patient, and the overall combination of findings that I’ve described in ECG #1— I thought the odds greatly favored this tracing to be a repolarization variant.
- IF the provider-at-the-bedside ever has any doubts about a diagnosis — then GET more information! (ie, more history — serial ECGs — serial troponin values — Echo at the bedside during chest pain). More information was sought — and, finding a prior ECG on this patient that looked the same as ECG #1 confirmed the findings of increased voltage + a repolarization variant.

Doesn't the st-t ratio differentiate acute pericarditis from stemi?
ReplyDelete@ Subhasish — No, the purpose of the ST-T Ratio is to distinguish between acute pericarditis and a repolarization variant. That said, as per my discussion — we are dealing with a differential diagnosis of 3 things = acute MI - repol variant - pericarditis. Hopefully my discussion provides a rationale for why I thought this case to most likely reflect a repolarization variant in a patient with LOTS of QRS amplitude in many leads! — :)
DeleteWouldn’t another differential diagnosis be pulmonary embolism? If not, why not?
DeleteI seem to recall it being mentioned in the case as an example, but I may have misunderstood.
Thank you
Tim K
@ Tim K — Reasons why ECG #1 does not suggest acute PE to me are: i) No tachycardia; ii) No ECG findings of RV “strain” (ie, no right axis, no RAA, no ST-T depression in inferior and/or anterior leads, no tall R in V1, no persistent precordial S waves); and iii) The tracing looks like a repolarization variant in a young adut with a lot of voltage.
DeleteHello. Aside from the topic, could you please recommend to me a blog about detailed echocardiography cases like this ECG blog? Reading echo textbooks doesn't help as much as discussed echo cases as this ECG blog helped me so much in understandig a lot of concepts in ECG. Thanks.
ReplyDelete@ Elyar. Drs. Smith & Meyers often comment on their bedside Echos in this Blog. Regarding other recommendations for "Echo Cases" — Dr. Smith's favorite is by Mike and Matt at ultrasound podcast (https://www.ultrasoundpodcast.com/category/podcast/ ). Another that Dr. Meyers recommends = https://www.emergencyultrasoundteaching.com/cases.html . I'll add that simple search on Google for "Echo Cases" brings forth a large number of links — but you'd have to check each of these out to see if they provide what it is you are looking for. BEST of LUCK — and hope the above is helpful — :)
Delete