
This patient who presented with acute heart failure has a history of heart failure and atrial fibrillation:
There is atrial fibrillation with a controlled ventricular rate. There is scooped ST depression in II, III, aVF and especially in V5, V6.
There are 4 categories of etiologies of ST depression in the context of a normal QRS:
1. Ischemia
2. Hypokalemia
3. Digoxin
4. Baseline/non-pathologic
--When the QT interval is very short, think digoxin.
--When the patient has atrial fibrillation with a controlled ventricular rate, it is not unlikely that the patient is on Digoxin for rate control.
--When the ST depression is what I call "scooped", think Digoxin.
When I suggested this as the likely etiology of the ST depression, and asked if she is on Digoxin, the resident said "That is so old school"!!
Well, it turned out she was on Digoxin, and there was no ischemia.
I showed this with no info to one of our young but very smart toxicology faculty and she instantly said "Dig", proving that this is not "old school."
Finally, it is important to remark that this is Dig effect and NOT Dig toxicity.
"Salvador Dali's mustache"
Some have likened the scooped ST depression of digoxin effect to "Salvador Dali's mustache" (for those of you who are young, Salvador Dali was the archetypal Surrealist painter).
This image comes from Life in the Fast Lane. I'm not sure they created it. https://litfl.com/digoxin-effect-ecg-library/




 |
| This was interpreted as "lateral ischemia". The patient's previous hospital admission had been predicated on this "ischemia." What do you think? |
There is atrial fibrillation with a controlled ventricular rate. There is scooped ST depression in II, III, aVF and especially in V5, V6.
There are 4 categories of etiologies of ST depression in the context of a normal QRS:
1. Ischemia
2. Hypokalemia
3. Digoxin
4. Baseline/non-pathologic
--When the QT interval is very short, think digoxin.
--When the patient has atrial fibrillation with a controlled ventricular rate, it is not unlikely that the patient is on Digoxin for rate control.
--When the ST depression is what I call "scooped", think Digoxin.
When I suggested this as the likely etiology of the ST depression, and asked if she is on Digoxin, the resident said "That is so old school"!!
Well, it turned out she was on Digoxin, and there was no ischemia.
I showed this with no info to one of our young but very smart toxicology faculty and she instantly said "Dig", proving that this is not "old school."
Finally, it is important to remark that this is Dig effect and NOT Dig toxicity.
"Salvador Dali's mustache"
Some have likened the scooped ST depression of digoxin effect to "Salvador Dali's mustache" (for those of you who are young, Salvador Dali was the archetypal Surrealist painter).
This image comes from Life in the Fast Lane. I'm not sure they created it. https://litfl.com/digoxin-effect-ecg-library/
- Steve — I believe Dale Dubin first popularized the image of Salvador Dali's mustache as a representation for the "scooped" shape of Digoxin effect (Ken Grauer, MD).

Some other interesting posts on Digoxin:
Looks like a Posterior STEMI. Is it?
 |
| This one is pathognomonic of Dig toxicity. There is an accelerated junctional rhythm Note the ST depression has a very short QT; hence cannot be ischemia |
Coved ST elevation with reciprocal ST depression: what is the diagnosis?
 |
| Here the scooped ST depression is in aVL. Note the very short QT |
ST segment depression: what is the etiology?

===================================
MY Comment by KEN GRAUER, MD (10/21/2019):
===================================
Excellent post by Dr. Smith to highlight potential causes of ST depression on ECG. While I immediately had the same initial thought about this case as Dr. Smith (ie, “Is this patient on Digoxin?” ) — I’d like to expand on his comments.
- For clarity — I’ve reproduced the 1st ECG shown in this case (Figure-1).
 |
| Figure-1: The 1st ECG shown in this case (See text). |
Pertinent points regarding the interpretation of ECG #1 include:
- Descriptive Analysis of the ECG Findings: The rhythm in ECG #1 is AFib with a fairly slow ventricular response (ie, the rate dips below 60/minute in several places). All intervals are normal (as per Dr. Smith — the QTc looks short). The frontal plane axis is normal at +60 degrees. There is normal standardization — and clearly no sign of ventricular hypertrophy by voltage. Regarding Q-R-S-T Changes — there are small septal q waves (in leads aVL, V6) — transition is slightly delayed (occurs between V4-to-V5) — with the most remarkable finding being appearance of ST-T waves.
- NOTE #1: This ECG was apparently “interpreted” as showing “lateral ischemia”. This “interpretation” suggests premature closure regarding the diagnostic possibilities — so there is little wonder that the correct diagnosis was initially overlooked. We are still in the Descriptive Analysis phase, rather than “interpretation”. The way in which I would describe ST-T wave appearance in this ECG is that there are, “diffuse, nonspecific ST-T wave abnormalities” with (as per Dr. Smith) — ST segment “scooping” with a short QTc, that is most prominent in the lateral chest leads.
- NOTE #2: More than just the infero-lateral leads — virtually all leads on this tracing (except perhaps aVR and V1) show ST-T wave abnormalities (if not ST “scooping” — then nonspecific ST-T wave flattening).
- Clinical Impression: Optimal interpretation of ECG #1 should indicate that there is AFib with a fairly slow ventricular response + nonspecific ST-T wave flattening that includes ST segment “scooping” with a short QTc in several leads. Clinical Correlation is then needed to assess which one (or more) entities is (are) most likely to be responsible for this ST-T wave appearance (Figure-2).
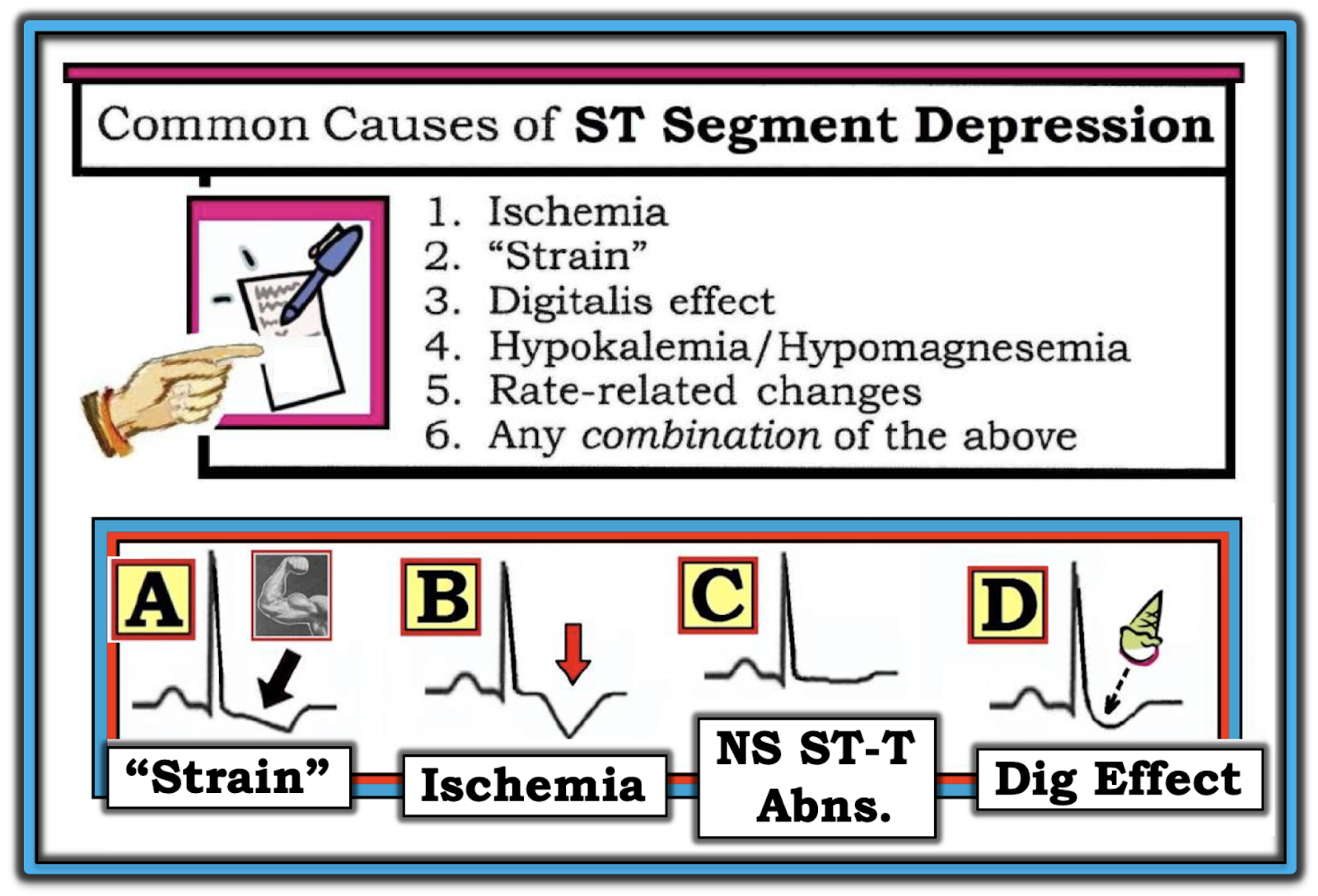 |
| Figure-2: Common causes of ST-T wave depression (See text). This Figure was taken from my ECG Blog #166. |
Causes of ST-T Wave Depression: There are actually over 50 causes of ST-T wave changes on ECG. Although many of these causes are cardiac-related — there are also many that are not cardiac-related. Among the many non-cardiac causes of ST-T wave changes are hyperventilation; temperature extremes (excessive heat or cold exposure); anxiety or emotional stress; anemia; tachycardia; sleep deprivation; pulmonary disease; electrolyte abnormalities; central nervous system disorders; certain medications; and severe medical illness (among others). KEY Point — Many of the 50+ potential causes of ST-T wave abnormalities on ECG are non-cardiac!
- BOTTOM Line: Rather than attempting to commit to memory an exhaustive list of conditions that may predispose to ST-T wave changes — it suffices to appreciate the variety of entities that may produce changes on ECG.
- NOTE #3: In general — causes of T wave abnormalities (including T wave flattening or frank T wave inversion) are similar to potential causes of ST segment depression.
We favor remembering the short LIST of entities that we show in Figure-2. Our purpose in making this List, is to simplify your task as the interpreter. As soon as you recognize generalized ST-T wave changes on an ECG — Consider the short LIST of Potential Causes in Figure-2:
- NOTE #4: Often — more than a single cause may be operative. For example — the patient in this case had a history of heart failure and AFib — so we can presume this patient was probably taking at least a few medications. As a result — the patient might be taking Digoxin and/or a Diuretic (which might contribute to electrolyte disturbance). The patient has heart failure — so the abnormal ST-T wave changes may reflect LV “strain” (or a strain equivalent). And despite a history of recent chest pain — the ST-T wave changes we see in ECG #1 could reflect chronic ischemia. BOTTOM Line — Except for tachycardia, each of the other potential causes of ST-T wave depression in Figure-2 might be contributing in varying degree to the ECG picture we see in Figure-1.
PEARL: The Shape of the ST-T wave may suggest which one (or more) of the 6 entities in our LIST is (are) most likely to be operative in a given patient (See bottom half of Figure-2):
- Ischemia — is suggested by symmetric T inversion (RED arrow in Panel B) — especially when seen in two or more leads of a given lead group (ie, in leads II, III and aVF — or in both leads I and aVL). Ischemia may also manifest ST segment flattening or depression — but other entities may produce this same picture. However, true symmetric T wave inversion in 2 or more leads in an anatomic lead area increase the chances of ischemia (acute or chronic) as the etiology.
- Strain — from LVH, is suggested by asymmetric ST depression occurring in one (or more) of the lateral leads (less often in the inferior leads). Note the initial slow sagging of the ST segment with LV “strain” (BLACK arrow in Panel A) — with more rapid return to the baseline. “Strain” is more likely to be the cause of ST depression when ECG voltage for LVH is present. NOTE #5: On occasion, there may be Echo-verified LV enlargement with ST-T wave changes suggestive of “strain” on ECG — but without accompanying voltage. This point may be relevant to the patient in this case — as asymmetric ST-T wave depression is most marked in lateral leads in this patient with chronic heart failure (that predisposes to LV enlargement) — but who does not satisfy any ECG voltage criteria for LVH in ECG #1.
- "RV strain" — is suggested IF the picture in Panel A of Figure-2 is seen in right-sided leads (leads II,III,aVF; or V1,V2,V3) in a patient with RVH.
Use of Digoxin may affect ST-T waves in any one of 3 ways: i) There may be “scooped” ST depression in multiple leads (that simulates an inverted ice cream cone, as in Panel D of Figure-2). This is often associated with a relatively short QTc; or, ii) Digoxin “effect” may produce a "strain"-like pattern (identical to Panel A); or, iii) Despite use of an appropriate amount of Digoxin — there may be little-to-no effect on the ST-T wave.
- NOTE #6: In my experience (from correlating ECG ST-T wave appearance to serum Digoxin levels over the 3 decades that I worked closely with PharmDs at our institution) — the serum Digoxin level correlates poorly with the amount of ST-T wave scooping or depression. Thus, despite even high serum Digoxin levels — some patients fail to manifest ST-T wave abnormalities — whereas other patients show marked ST-T wave changes despite surprisingly low serum Digoxin levels.
Finally — Panel C in Figure-2 shows a non-specific ST-T wave pattern, in which the T wave and ST segment are flattened (if not slightly depressed). This pattern is called “nonspecific” — because any of the many potential causes of ST-T wave abnormalities may be operative.
BOTTOM Line (regarding ST-T wave changes in ECG #1 for this case) = Clinical correlation is needed:
- As per Dr. Smith — the “scooped” ST segment appearance in several leads (most remarkable in leads III, V5, V6) with noticeably shortened QTc make inquiring about whether the patient is on Digoxin the 1st priority.
- That said — the other entities on the LIST in Figure-2 should also be considered — as they may be contributing to the ST-T wave changes we see. Reviewing the patient’s medication list — serum electrolyte values (especially serum K+ and Mg++) — and, obtaining a prior ECG for comparison purposes would all be helpful.
- The “good news” in this case — is that the ST-T wave changes we see in Figure-1 do not look acute. In the absence of a history of worrisome, new-onset chest pain — it is highly unlikely that the ST depression in ECG #1 reflects acute ischemia.
A good example of "scooped-out" ST segment of digitalis effect. Also, very important to point out, as you did, that this is not a sign of digitalis toxicity but just a pharmacological effect of digitalis.
ReplyDeleteK. Wang.
Thanks (as always!) K for you comment — :)
Delete