
Case submitted and written by Alex Bracey, with edits by Pendell Meyers
A man in his 50s without prior medical history was sent to the emergency department from an urgent care facility for concern of an "abnormal ECG" after he had complained of chest pain earlier in the day. He was symptom free at the time of arrival.
ED ECG#1
 |
| What do you think? What do you think his urgent care ECG (done during pain) will show? |
This ECG shows sinus bradycardia with terminal ST depressions in II, III, aVF, V3-V6, with reciprocal changes in aVL and I. These findings indicate reperfusion of the inferior and lateral walls, implying that an ECG during active symptoms would likely show OMI.
Note: This is the same pathophysiology and electrophysiology involved in Wellens syndrome, which is simply the name given to reperfusion of anterior wall OMI when the patient is in the pain free state of reperfusion and has not yet lost the anterior wall (requires persistent R-waves to be classic Wellens syndrome). This pattern occurs in any wall of the heart, whichever wall is currently reperfused from a prior occlusion.
On this note, "type A" and "type B" Wellens are useless distinctions that arose before we realized that reperfusion is a progression of findings starting with terminal T-wave inversions ("type A") and progressing to full T-wave inversions ("type B"). My analogy for this misunderstanding of Wellens syndrome that I tell my residents is this: "Imagine you were an alien looking through a microscope and you discovered Earth. You zoom in to a city and look at a single street and you see humans, which happens to be a woman walking with her small child. You watch them for a few hours and then report your findings to your fellow aliens: you declare that there are two types of humans: type A (smaller, helpless ones) and type B (large, smarter ones). If they simply had more knowledge and experience with humans, it would be easy to understand that type A and type B are not different types at all, rather different points along the same progression. If you only look at individual snapshots in time, they appear to be different types, however if you follow them for the full course of their progression the pattern becomes clear.
On this note, "type A" and "type B" Wellens are useless distinctions that arose before we realized that reperfusion is a progression of findings starting with terminal T-wave inversions ("type A") and progressing to full T-wave inversions ("type B"). My analogy for this misunderstanding of Wellens syndrome that I tell my residents is this: "Imagine you were an alien looking through a microscope and you discovered Earth. You zoom in to a city and look at a single street and you see humans, which happens to be a woman walking with her small child. You watch them for a few hours and then report your findings to your fellow aliens: you declare that there are two types of humans: type A (smaller, helpless ones) and type B (large, smarter ones). If they simply had more knowledge and experience with humans, it would be easy to understand that type A and type B are not different types at all, rather different points along the same progression. If you only look at individual snapshots in time, they appear to be different types, however if you follow them for the full course of their progression the pattern becomes clear.
To make type A and B even more useless, they are misnomers applied by someone who had not carefully read Wellens' papers. They called terminal T-wave inversion type B and deep inversion type A. Wellens called terminal T-wave inversion "Pattern A" and deep "Pattern B."
He reports that today while sitting outside he developed sudden onset bilateral arm “burning” and an “odd feeling” though he was not able to further describe it. He had no chest pain, heaviness, or discomfort at any point and was never short of breath during today’s events. When pressed, he recalls that last week he traveled to Denver where he experienced dyspnea on exertion, though he attributed it to the altitude.
Urgent Care ECG (this was done before arrival to ED, during active symptoms):

STE in II, III, and aVF (which probably barely does meet STEMI critiera) with hyperacute T waves in II, IIII, aVF and reciprocal negative hyperacute T-wave in aVL, with STD in V1-V2
Small R waves in II, III, aVF
This is diagnostic of inferoposterior OMI. The most likely culprit vessel would be the RCA.
Back to the present, in the ED, asymptomatic:
Given that the patient was now asymptomatic in the ED with ED ECG#1, I asked for serial ECGs to be recorded every 30 minutes and for any acute changes in discomfort or clinical condition.
At our facility we have a process to promptly evaluate patients for urgent or emergent PCI that present with ECGs concerning for acute coronary occlusions that do not meet STEMI critieria (OMI) called Heart Alert. We activated this process and the cardiology fellow presented to the bedside.
A third ECG was record at this time with no change, persistent reperfusion pattern.
During this time I received a call from the interventional cardiologist. I discussed the case with him as he reviewed the ECG. We agreed that there were dynamic changes; however, he did not feel that it could represent acute coronary syndrome as the patient did not have chest pain at any time during his prior symptoms.
During this time I received a call from the interventional cardiologist. I discussed the case with him as he reviewed the ECG. We agreed that there were dynamic changes; however, he did not feel that it could represent acute coronary syndrome as the patient did not have chest pain at any time during his prior symptoms.
This is clearly false.
The patient then reported another episode of diaphoresis. An ECG at this time was recorded:


Redemonstration of small STE in II, III, aVF (not meeting criteria in this ECG) and reciprocal changes in aVL, V2. This ECG demonstrates reocclusion of the affected coronary vessel.
At this time the cardiology fellow again contacted the interventionist who agreed to take the patient for urgent PCI at this time.
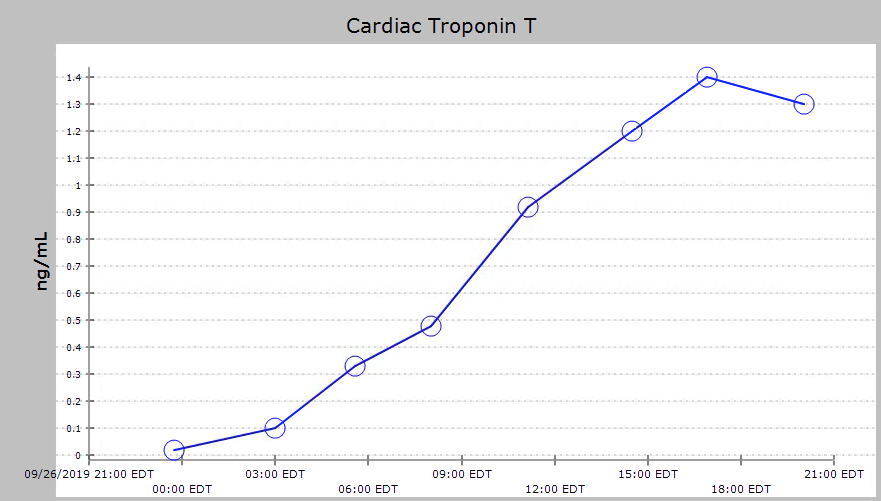
His initial troponin T was 0.02 ng/mL.
Here is what they found on cath:
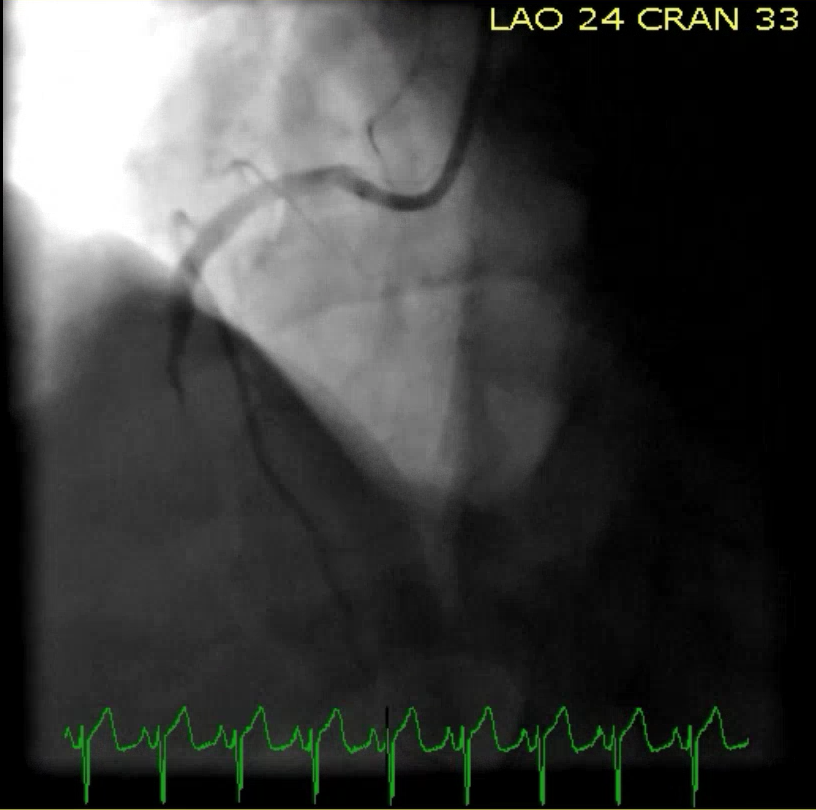 |
100% mRCA with TIMI 0 flow
|
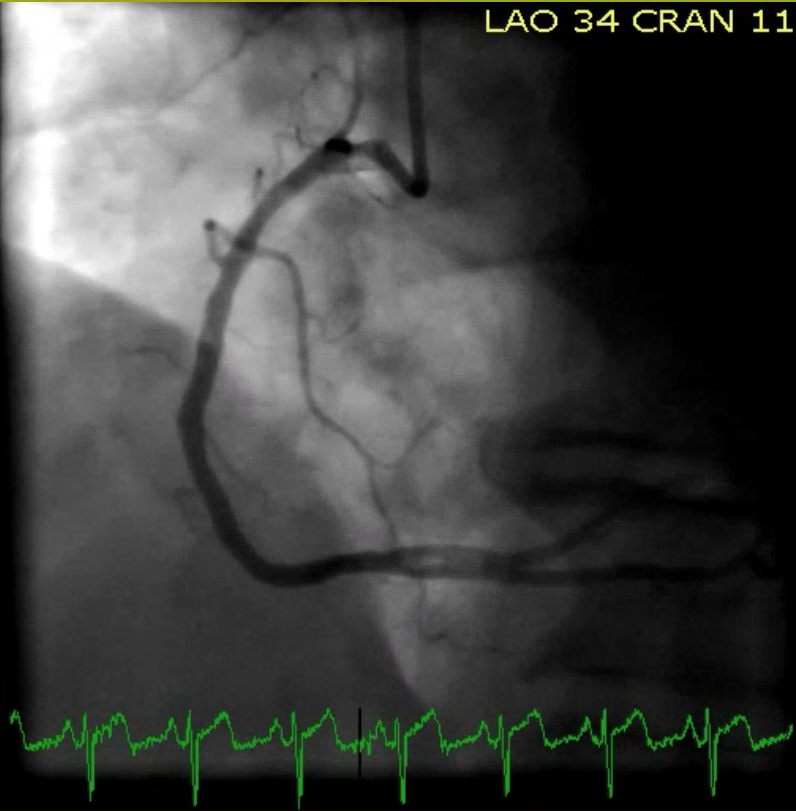 |
Post DES RCA with TIMI 3 flow
|
His formal echo performed the next day revealed an EF of 50% and Septal, lateral, and apical wall motion abnormalities.
His troponin T continued to climb over the next day with a peak of 1.4 ng/mL.
He had an uncomplicated post-PCI course and was discharged 3 days later.
Teaching Points:
We must understand the ECG patterns of occlusion and reperfusion because they are not currently taught or understood in the classic STEMI paradigm.
We must understand the ECG patterns of occlusion and reperfusion because they are not currently taught or understood in the classic STEMI paradigm.
Serial ECGs greatly increase the chances of finding diagnostic features of OMI on ECG.
===================================
MY Comment, by KEN GRAUER, MD (10/10/2019):
===================================
Highly insightful case! Drs. Bracey and Meyers have intentionally changed the time sequence in which the tracings in this case were recorded in order to make a number of important points.
- I limit my comments to discussion of the 1st ECG shown above. This is the initial ECG that was done at the time the patient arrived in the ED.
- I will offer a different perspective on the interpretation of ECG #1. For clarity — I have reproduced and labeled this ECG in Figure-1.
 |
| Figure-1: The initial ECG done in the ED (See text). |
I propose the following additional Teaching Points regarding interpretation of ECG #1, considering the clinical context in which this patient presented:
- Although I was not surprised by ECG findings on the Urgent Care ECG (which was the 2nd ECG shown above) — I do not think ( = my opinion) that there was any way to be certain there was ongoing acute infero-postero OMI from assessment of ECG #1 alone.
- From an ECG Learning perspective — Systematic interpretation of ECG #1 should result in recognition of at least 4 additional findings not mentioned above. Admittedly, recognition of these findings does not alter management in this case — but there are times when failure to routinely use a systematic approach will result in overlooking ECG findings that are important (as I have shown on prior posts).
At the time ECG #1 was obtained in the ED — all that the ED physician knew was the HISTORY (a 50s man who was previously healthy, had chest pain earlier that day — but was asymptomatic at the time ECG #1 was done). Systematic Interpretation begins with Descriptive Analysis (I’ve put additional findings that should be recognized in BOLD).
- Rate & Rhythm — There is sinus bradycardia (rate in the 50s, perhaps with some sinus arrhythmia).
- Intervals (PR/QRS/QT) — The PR interval is normal. The QRS complex is narrow. The QTc is not prolonged.
- Axis — There is marked left axis deviation — with a predominantly negative QRS in lead II (ie, the axis is more negative than -40 degrees). This is consistent with LAHB (Left Anterior HemiBlock). We don’t know if this is a new finding ...
- Chamber Enlargement — There is no atrial enlargement, and no RVH. But criteria for LVH are met! (ie, R in lead aVL≥12 mm).
Q-R-S-T Changes:
- Q = There are small (normal septal) q waves in leads I and aVL.
- R = There is something strange about R wave progression! There may be a tiny q wave in lead V2? Abrupt transition from the negative QRS in lead V1 — to the predominantly positive QRS complex by V2 — with then loss of R wave by V3, just doesn’t make physiologic sense. Note a much more logical progression of QRS and ST-T wave morphology across the chest leads for the other 2 ECGs done in this case. Recognition that placement of lead V2 may be off in ECG #1 is relevant in this case, given the ultimate evolution of acute infarction.
- ST-T Wave Changes — As emphasized by Drs. Bracey and Meyers, there is terminal T wave inversion in multiple leads in ECG #1 (BLUE arrows highlight this in leads V3 and V4 — but it is also present in leads II, aVF, V5 and V6). As was also emphasized — this ECG finding of a biphasic T wave with terminal T wave inversion (and with frank T wave inversion in lead III) alerts us in a patient with chest pain earlier that day — to the strong possibility that these findings may reflect reperfusion changes. (PINK — then BLUE arrows, highlight the biphasic nature of these T waves.) That said, there really is no ST elevation, no ST depression, and no non-septal Q waves in ECG #1 — and, in the absence of a prior or subsequent tracings — I don’t think ( = my opinion) that a definitive diagnosis of acute infarction can be made. We simply have NO idea as to when these ECG abnormalities may have developed … These ECG changes could certainly be acute — or, they may have developed days (or longer) before ECG #1 was done.
- That said — it should be noted that in addition to these biphasic T waves with terminal inversion (and the frank T inversion in lead III) — ST segments just before these T waves are inappropriately flat in multiple leads (short horizontal BLUE lines in Figure-1). This loss of the normal gradual ST segment upslope is a distinctly abnormal ECG finding, especially in a patient with recent chest pain.
BOTTOM LINE: It should be appreciated that other than leads aVR and V1 — the remaining 10 leads in ECG #1 all show abnormal ST-T wave findings. In a previously healthy middle-aged adult who experienced new chest pain earlier in the day — the overall assessment of ECG #1 alone should clearly justify timely cardiac catheterization.
- Once the earlier ECG from the Urgent Care Center became available — the diagnosis of acute ongoing infero-postero OMI became obvious. But, I thought it important to highlight all of the ECG findings that should be noted on ECG #1 — and, to emphasize that even if no Urgent Care Center ECG had been done, that timely cath would still be indicated.
Our THANKS to Dr. Bracey and Meyers for this insightful case!
Mind blowing analysis by Dr. Ken. Thank you
ReplyDeleteTHANKS so much for the kind words. I believe it is a highly insightful case! — :)
DeleteA very interesting and important ECG. My thanks to Drs. Bracey, Meyers and Grauer. My first impression from the initial ECG presented (done in the ER) was that you were dealing with reperfusion T waves and a Wellens-type syndrome. I was suspicious that this was a momentary occlusion of a distal type 3 ("wraparound") LAD because of the involvement of V3 (which also follows the conventional thought that Wellens syndrome is an LAD phenomenon). V3 is a bit far for the LCX or RCA to reach (but obviously not impossible for the RCA, since it is capable of affecting V1 - V6). The ECG done at the urgent care facility, however, was clearly an acute inferior epicardial ischemia with lateral wall extension. STD in V1 - V3 represents a lateral wall epicardial ischemia. The "true" posterior wall of the heart faces the right shoulder and will typically manifest infarctions as conduction delays or notching in V3 and V4 (probably mostly V4). Since V2 - V6 appear to have been involved at different points, this appears to be an occlusion of a superdominant RCA distal to the RV branches (sometimes referred to as a "mega-artery").
ReplyDeleteTHANKS Jerry! Excellent points that you bring up — :)
DeleteIn my post I mention that what we used to call a "posterior" MI is actually a LATERAL WALL MI. I created a short video demonstrating why this is so and posted it on YouTube (https://www.youtube.com/watch?v=46_G0SFgSTc). It's also on my profile page on LinkedIn and it is also a recent post on LinkedIn.
DeleteIf you have a moment, take a look at it. Although it is animated, nothing will move for about the first minute or so while I discuss a few preliminary concepts. I hope you enjoy it!
Thanks so much Jerry! The link that you left works (just paste and click!). NICE video — :)
DeleteI am posting the following comment from Dr. Stephen Smith: Jerry — I have long been aware of this work by Bayes de Luna. In my opinion — it is not helpful electrocardiographically. There is an important difference between: i) ECGs that have ST depression in V2 and V3 (and, if one were to place posterior leads, probably also in V7-V9); vs ii) ECGs that have ST elevation in V5, V6, or I, aVL. Although Bayes de Luna has shown that the actual myocardial wall is "lateral" by his methods, it has no relevance to analyzing an ECG. I oppose this framework, as it makes it more difficult to treat OMIs that only have ST depression — Steve
Deleteextraordinary.
ReplyDeleteit is always a pleasure watching great minds, as illustrated by the four of you , alex, pendell, ken , and dr jones, dissect analyze, and explain the intricacies of an interesting case, and set of ecg's.
i am often discouraged by the fact that our cardiology colleagues are often , even at major sites, so hesitant to act upon very concerning, non-"in-your-face-STEMI" ecgs. in 2019 (not 1919).
maybe next year.
thank you guys.
tom
THANK YOU Tom! In this particular case — there is mention of a cardiology Fellow, who apparently initially saw the case — and was in contact with his/her Attending … — so I can’t tell from the information given what the experience of the cardiology Fellow consultant was … We also don’t know from the history given whether the Attending Cardiologist initially got the whole story (including the ECG from the Urgent Care Center) — or just received brief verbal report. BOTTOM LINE: We are ALL learning every day — and my hope is that BOTH that cardiology Fellow AND the Attending Cardiologist LEARN from this case. I will never forget early on in my Attending career receiving a call from the Resident on call, in which I didn’t insist on seeing the actual ECG — and as a result, the correct diagnosis was delayed. I quickly learned the importance of insisting “Show Me the ECG you are talking about”. These days with cell phones — it takes seconds to copy a tracing … THANKS (as always!) for you comments — :)
Delete