
This is written by Brooks Walsh.
https://twitter.com/BrooksWalsh
It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back.
She had given birth a week ago, and she had similar chest pain during her labor. She attributed the chest pain to anxiety and stress, saying "I'm just an anxious person."
https://twitter.com/BrooksWalsh
A 30 year-old woman was brought to the ED with chest pain.
It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back.
She had given birth a week ago, and she had similar chest pain during her labor. She attributed the chest pain to anxiety and stress, saying "I'm just an anxious person."
A CXR and a CTA for PE were normal.
The ECGs
An initial ECG was obtained as the pain was rapidly resolving:
 |
Minimal upsloping ST Elevation in III, with a steeply biphasic T wave, and with reciprocal ST depression in leads I and aVL.
There is also a Q-wave in III. This strongly suggests reperfusing RCA ischemia.
There is also subtle STD in V3-V5.
(Inverted T in V2 is likely due to lead misplacement -- this is evidence by the inverted P-wave) |
A second ECG was obtained 6 hours later (pain-free):
 |
| Aside from a slightly biphasic T wave in lead III, the findings from the first ECG are now resolved. |
This dynamic findings, especially when correlated with the patient’s resolving symptoms, are not “non-specific.” The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. The initial STD depression in aVL and V3-V5 (later resolved) further supports a very recent occlusion affecting this area.
Troponins, echocardiogram
An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia, likely of the area supplied by the RCA.
The initial troponin I was elevated at 0.75 ng/ml (99th %-ile URL = 0.04 ng/ml), and rose to 12 ng/ml six hours later. This rate and height of troponin rise strongly suggested a type 1 MI.
Angiography was performed after aspirin and heparin were started.
Here’s the angiogram of the RCA:
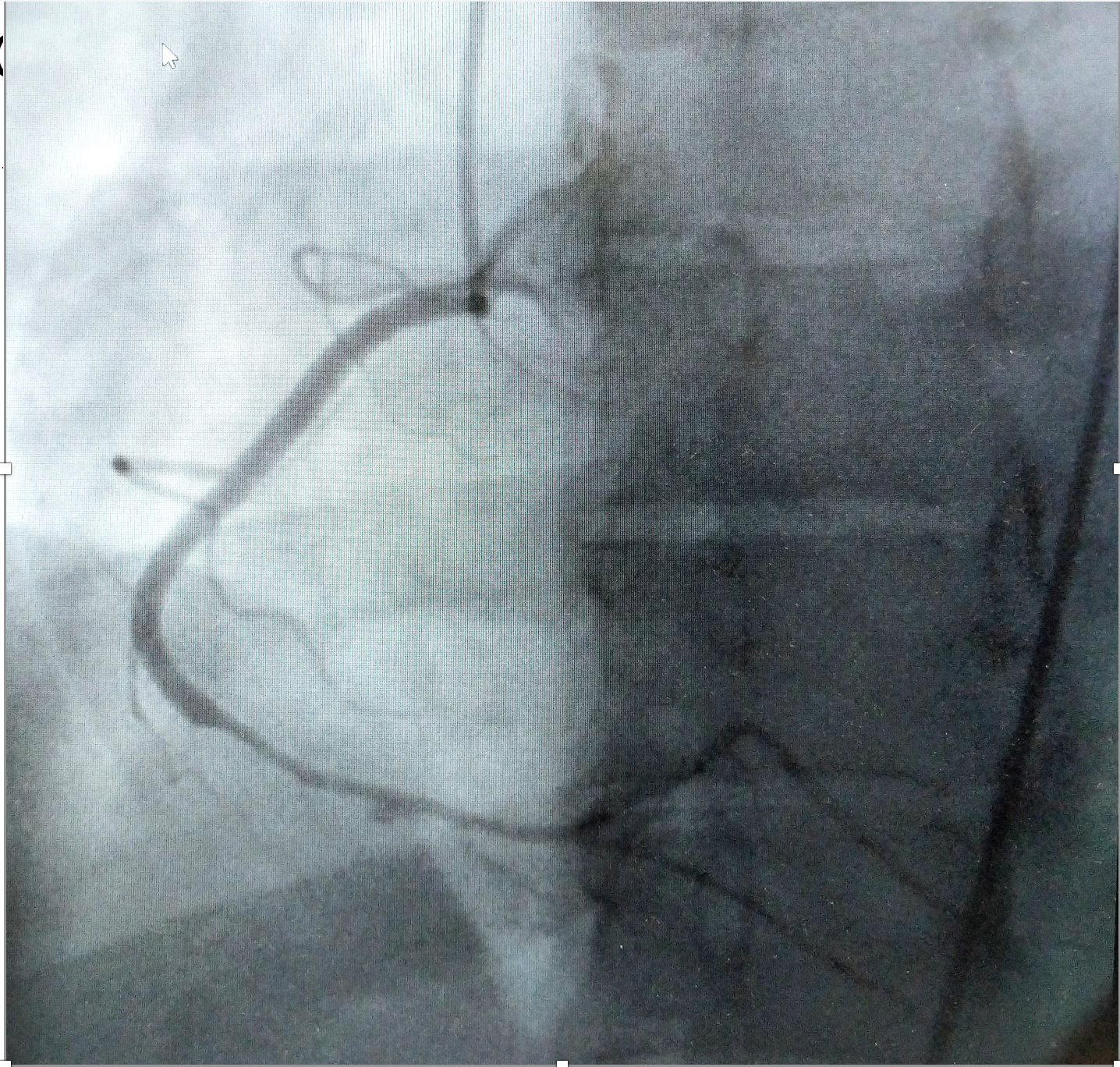
No thrombus or plaque rupture in the RCA (or any coronary artery) was found.
However, a smooth tapering of the mid-RCA was seen, highlighted in red below:
However, a smooth tapering of the mid-RCA was seen, highlighted in red below:
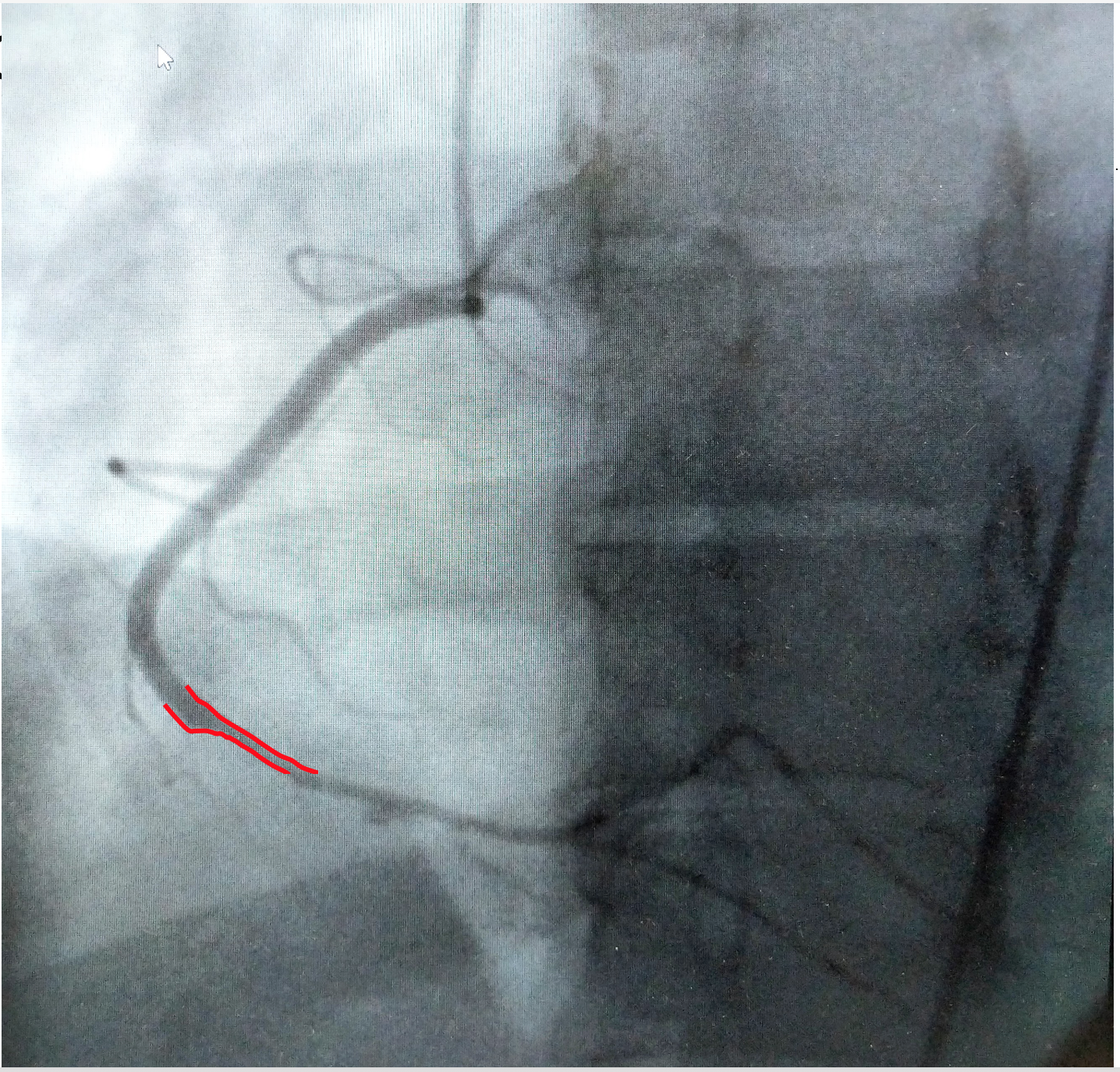
How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Spontaneous coronary artery dissection
Dissection of a coronary artery may occur in the context of atherosclerosis, or be iatrogennic during angiography or angioplasty. In the absence of these factors it is termed spontaneous coronary artery dissection (SCAD).
This case occurred 10+ years ago. At that time the literature suggested:
- SCAD was rare,
- Mostly related to pregnancy,
- Seen on angiography as a dissection flap, and
- Managed similarly to MI caused by CAD (ASA, BB, lytics/PCI).
An athletic 30-something woman with acute substernal chest pressure
Five takeaways about SCAD:
1. SCAD isn’t rare, especially in women
Historically SCAD had been identified in < 1% of angiograms performed for ACS. However, contemporary studies find it in up to 4% of ACS, and in > 22% of ACS cases in women. A recent study found that SCAD causes almost 20% of STEMI in young women.
2. Pregnancy is not a common cause of SCAD
When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. However, pregnancy-associated spontaneous coronary dissection (PA-SCAD) is still pretty uncommon, and accounts for less than 5% of SCAD cases overall. Fibromuscular dysplasia is a much more common trigger for SCAD.
3. SCAD can have subtle angiographic features, and coronary CTA is unhelpful.
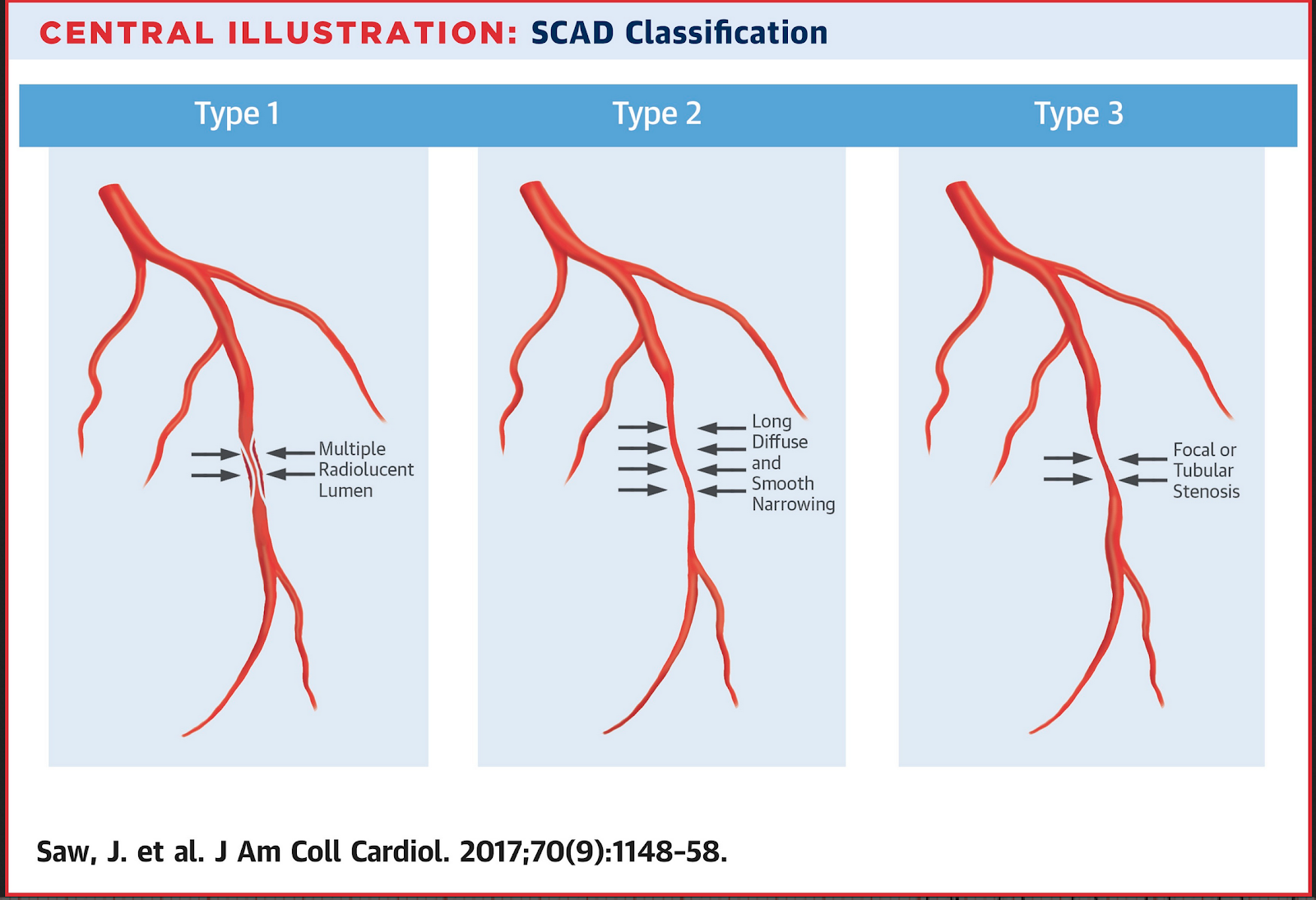
SCAD was originally thought to show a characteristic dissection flap and and false lumen(s) ion angiography. However, this “classic” pattern ( “Type 1”) only occurrs in about 25% of cases. Most SACD does not create a flap, and shows instead a long smooth narrowing of the true lumen. Type 2 is seen in almost 70% of cases. Our patient had a type 2 lesion.
Type 2 is more difficult to appreciate on angiography than type 1. The relatively poorer resolution of cardiac CTA makes it especially inappropriate to rule out SCAD. Often, intravascular ultrasound or intravascular optical coherence tomography is requeried to make the diagnosis.
4. You don’t just treat it like ACS caused by CAD
Aggressive intervention may cause more problems than the original SCAD lesion. Guidewires for PCI may be difficult to thread through the weak, twisty arteries, and may rupture the false lumen. Heparin hasn’t been shown to help or hurt, but could theoretically promote expansion of an intramural hematoma. Fibrinolytics have been associated with devastating complications. While there isn’t good evidence that aspirin and beta-blockers help, there are few concerns about their safety, and they are generally recommended.
5. Coronary lesions often resolve without intervention, but PCI has role
Treatment of SCAD requires a different risk-benefit calculation than ACS caused by typical atherosclerotic disease, as shown by two studies form this year.
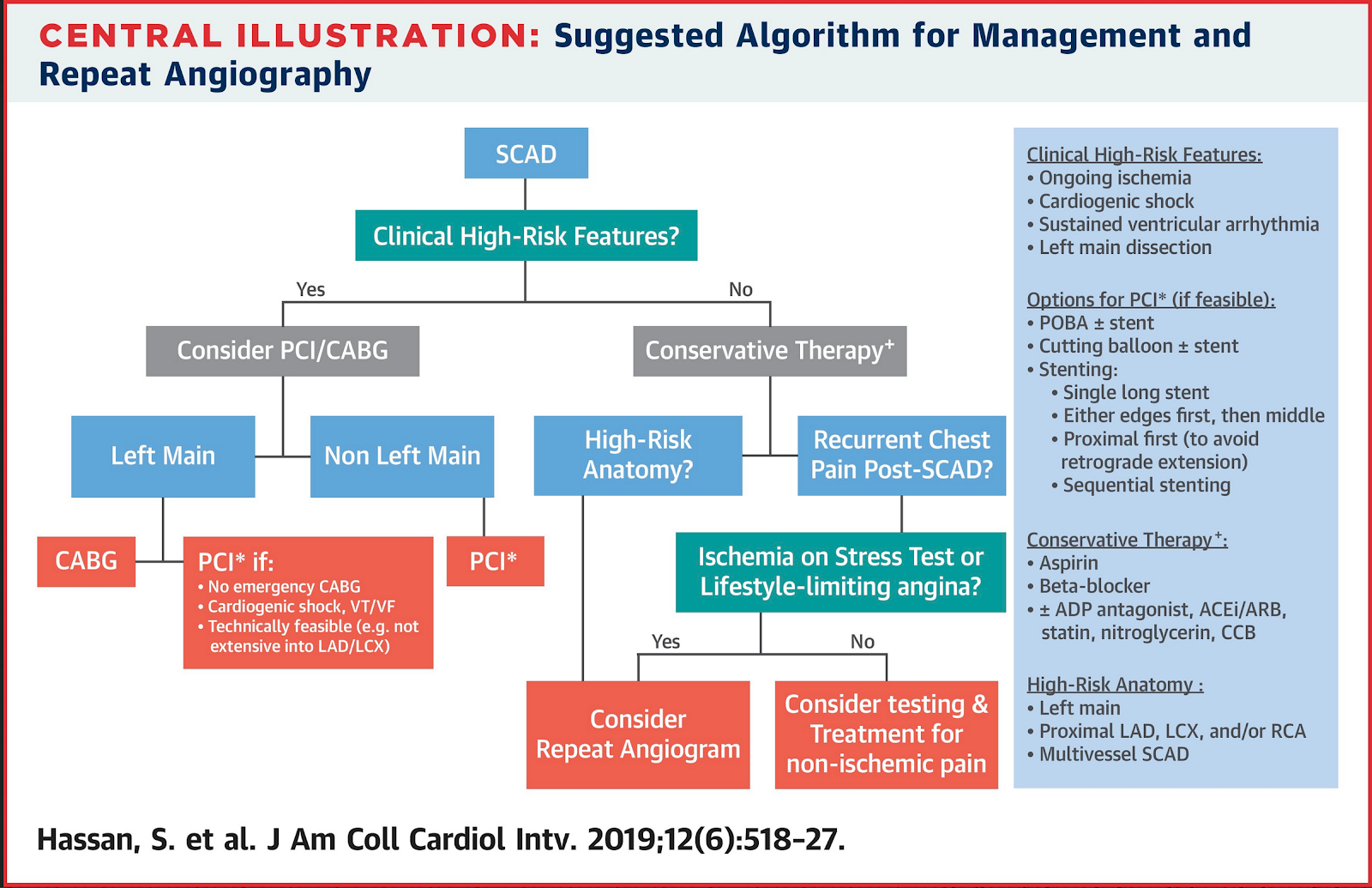
On the one hand, most SCAD lesions resolve with only conservative treatment, and PCI is not required. A study by Hassan et al. provided evidence that PCI/CABG was unnecessary for most SCAD, and should be considered for only high-risk presentations.
On the one hand, most SCAD lesions resolve with only conservative treatment, and PCI is not required. A study by Hassan et al. provided evidence that PCI/CABG was unnecessary for most SCAD, and should be considered for only high-risk presentations.
On the other hand , high-risk lesions appear to do well with aggressive treatment. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al. where more than 3/4 of cases were NSTEMI). The SCAD cases in Lobo et al. were pretty sick, with mostly LM/pLAD lesions and high rates of cardiogenic shock. Despite this, there was a high rate of PCI success.
Outcome of our case
Outcome of our case
Once the type 2 SCAD was identified, the heparin drip was stopped. No PCI was performed, and only conservative medical therapy was pursued. No evidence of a connective-tissue disease such as FMD was found. She did well, and was ultimately discharged from her cardiologist’s care years later!
References
Lobo AS et al. Revascularization in Patients With Spontaneous Coronary Artery Dissection and ST-Segment Elevation Myocardial Infarction. JACC 2019 Sep 10;74(10):1290-1300.
Hassan S. et al. Natural History of Spontaneous Coronary Artery Dissection with Spontaneous Angiographic Healing. JACC Cardiovascular Interventions 2019 Mar 25;12(6):518-527.

Hassan S. et al. Natural History of Spontaneous Coronary Artery Dissection with Spontaneous Angiographic Healing. JACC Cardiovascular Interventions 2019 Mar 25;12(6):518-527.
===================================
MY Comment, by KEN GRAUER, MD (10/24/2019):
===================================
Superb case by Dr. Brooks Walsh regarding the entity of SCAD (Spontaneous Coronary Artery Dissection). I had no idea SCAD was so common a cause of acute STEMI in younger women, even when they are non-smokers ..
Excellent description by Dr. Walsh of the ECG findings in the 2 tracings provided in this case! KEY to assessment of these findings is appreciation of the changes between these 2 tracings. I find putting these 2 tracings together greatly facilitates interpretation (Figure-1).
 |
| Figure-1: The 2 ECGs in this case (See text). |
MY Thoughts on the ECGs in Figure-1:
The patient in question was a 30-year old woman who had given birth 1 week earlier. Her chest pain was a severe, non-pleuritic “pressure” that radiated to her back. A similar episode had occurred a week earlier during labor. ECG #1 was the initial ED tracing, obtained when her chest pain was rapidly resolving (Figure-1). I’d add the following thoughts to Dr. Walsh’s comments:
- ECG #1 differs from the usual picture of acute reperfusion following RCA occlusion — in that only 1 of the 3 inferior leads ( = lead III) suggested to me a recent acute event. Leads II and III are not normal (ie, they show ST segment straightening and slight J-point depression) — but I was not at all certain about an acute event from my initial review of this tracing.
- That said — the SHAPE of the ST-T wave in lead III (showing ST segment straightening with slight elevation + sharp downslope of the T wave leading to terminal T wave inversion) is very concerning. It is the finding of a near mirror-image opposite ST-T wave picture in lead aVL + the decidedly abnormal ST segment straightening with slight depression, leading to angulation at the onset of the T wave in lead I — that should convince us of something acute until proven otherwise!
- More than just a Q wave in lead III in ECG #1 — we see an initial Q — followed by rise to a small-amplitude R wave just above the baseline — followed by an S wave. This type of fragmented QrS pattern that we see in lead III supports the possibility that the tiny q waves in the other 2 inferior leads (II and aVF) may indeed be markers of infarction.
- As per Dr. Walsh — there is subtle ST-T wave flattening with slight ST depression in leads V3-thru-V6. While important to note — I felt these changes to be nonspecific.
- Reasons why Dr. Walsh thought the T wave inversion in leads V1 and V2 was probably due to lead misplacement (placement of these leads 1 or 2 interspaces too high on the chest) — include: i) There is a prominent negative component to the P wave in leads V1 and V2; ii) There is a definite rSr’ in lead V1, and suggestion of an r’ component also in V2; and, iii) QRST morphology of lead V1 strongly resembles that in lead aVR (CLICK HERE — and look to My Comment at the bottom of the page in the November 4, 2018 SSmith Blog for more detailed discussion of how to quickly recognize too high placement of leads V1 and V2 on the chest).
- BOTTOM LINE re ECG #1: While certain ECG features of acute MI are lacking in ECG #1 — the appearance of leads I, III and aVL — in association with subtle ST-T wave flattening with slight depression in many other leads, should clearly raise suspicion of an acute and/or recent cardiac event. Armed with new knowledge from Dr. Walsh that SCAD is surprisingly common as a cause of ACS (Acute Coronary Syndrome) among young women in the peripartum period — I will immediately include SCAD in my differential the next time I encounter a similar set of circumstances.
Comparing ECG #2 (obtained 6 hours later when the patient was pain-free) — with ECG #1:
- Lead placement looks better in leads V1 and V2. The terminal r’ is no longer seen in these leads — and although there is ST flattening, there is no longer T wave inversion in lead V2. Neither lead V1 nor V2 looks at all like lead aVR in ECG #2.
- Lead-by-lead comparison of ECGs #1 and #2 shows definite improvement. Although a q wave persists in lead III — the fragmented Q wave appearance in lead III of ECG #1 is no longer seen. Subtle J-point depression in many leads has resolved.
- NOTE: ST-T waves are still not normal in ECG #2. In addition to shallow T wave inversion in lead III — note distinct ST segment flattening in leads I, II, aVL, aVF, V2, V5 and V6. In isolation — I would interpret these ST-T wave changes we see in ECG #2 as “non-specific”. However (as per Dr. Walsh), in the context of comparison with ECG #1 — this improvement that we clearly see in ECG #2 at a time when chest pain has now totally resolved suggests dynamic ECG changes — and, in a patient with new chest discomfort — dynamic ECG changes tells us to assume an acute cardiac event until proven otherwise. This was confirmed by Echo, serum markers and cath.
Once again, our THANKS to Dr. Walsh for presenting this case!
Dr Smith
ReplyDeleteIt appears that there is little R wave progression from V2 to V3 and even decreases on V4. Would you consider these findings non-specific for this type of case or would they add to other findings discussed?
Regards
@ Brian — THANKS for you comment. I assume you are talking about the initial ECG in your question? ( = ECG #1 in Figure-1 in My Comment above). As I discussed in My Comment — leads V1 and probably also V2 in ECG #1 have probably been placed too high on the chest (Please check out the link I provide in my comment when I discuss this — as it highlight the 3 quick clues to V1,V2 misplacement). As a result — there is little one can conclude from R wave progression in ECG #1, when lead placement is almost certainly erroneous. Although lead placement is better in ECG #2 — I would not have expected BOTH the R wave and S wave in lead V2 to be taller than what we see in both V1 and V3 of ECG #2 — so there might also be some lead misplacement in ECG #2. The problem in assessing R wave progression is ALWAYS one of weighing the likelihood of at least some lead malposition (which is MUCH more common than is generally appreciated!) — vs what is “real”, in which case what is “real” due to “other factors” (ie, body habitus) vs true “loss of R wave” due to infarction. This is often a judgment call, about which one develops a “sense” for the likely cause of suboptimal R wave progression for the case at hand. In this case — I attributed the less than optimal R wave progression in both tracings as probably the result of lead malposition + some “delayed transition” that was NOT due to infarction (loss of myocardium). If interested — I discussed assessment of R wave progression in detail in my video on QRST Changes — Listen to the next ~12 minutes, starting from this link — https://youtu.be/vRgnVuRmiyI?t=1029 — and then let me know if you have additional questions! Thanks again for your comments! — :)
DeleteThank you Dr Grauer..
Delete