
Case submitted and written by Alex Bracey
A man in his 50s with no significant past medical history presented from a local beach with epigastric "burning" pain that had been intermittent for 4 days until this morning when it became constant at rest. He had associated nausea and diaphoresis, but overall looked well and had arrived by private vehicle to front triage. An ECG was performed there and brought to me for review:
 |
| What do you think? |
STE in V2-4 that might just barely meet STEMI criteria
STE in aVL, and to a lesser extent lead I
Obvious reciprocal STD in II, III, aVF
Regardless of whether this ECG truly meets STEMI criteria, it is obviously diagnostic of OMI, most likely LAD occlusion. There is possible beginning of terminal T-wave inversion in V4 -5 possibly suggesting some reperfusion, but overall the ECG clearly shows active occlusion.
Since it was on the border of meeting STEMI criteria, a "heart alert" was activated. The heart alert pathway at my hospital summons a cardiology fellow and interventionalist to review the case and ECG without yet activating other cath lab staff, thereby allowing for rapid evaluation of the need for PCI without additional resource utilization.
The cardiology fellow presented to the bedside and reviewed the following additional ECG that had been obtained just before his arrival:
 |
| STE still present in V2-V4 and aVL, but to a lesser extent than the initial Developing terminal T-wave inversion in V2-5, I, and aVL, implying reperfusion |
He proceeded to review the ECGs and the case. He inquired as to the patient's recent alcohol intake, which had been increased compared to usual as he was on vacation. He had discomfort with deep palpation of the epigastrium.
At this point the fellow was concerned but not convinced that the presentation and findings truly represented OMI and wanted to wait for a troponin level before activating the cath lab.
The patient continued to have pain despite the reperfusion pattern, so we administered heparin 4000 U IV in addition to aspirin.
At our facility, we unfortunately do not yet have access to emergent high quality contrast enhanced echocardiography for our heart alert cases. So we immediately performed a bedside echo.
Despite imperfect quality, this shows severe hypokinesis of the anterior wall with reduced LV function.
I reviewed the images with the cardiology fellow who agreed that the constellation of symptoms and findings was concerning enough to activate the cath lab at this point. No troponin had yet resulted.
There was only a delay of perhaps 20 minutes between our diagnosis of OMI and the cardiologists' decision to take him for emergent cath.
 |
| Pre intervention: proximal to mid-LAD 100% occlusion (TIMI 0 flow). |
 |
| Post intervention: stent placement with resultant TIMI 3 flow |
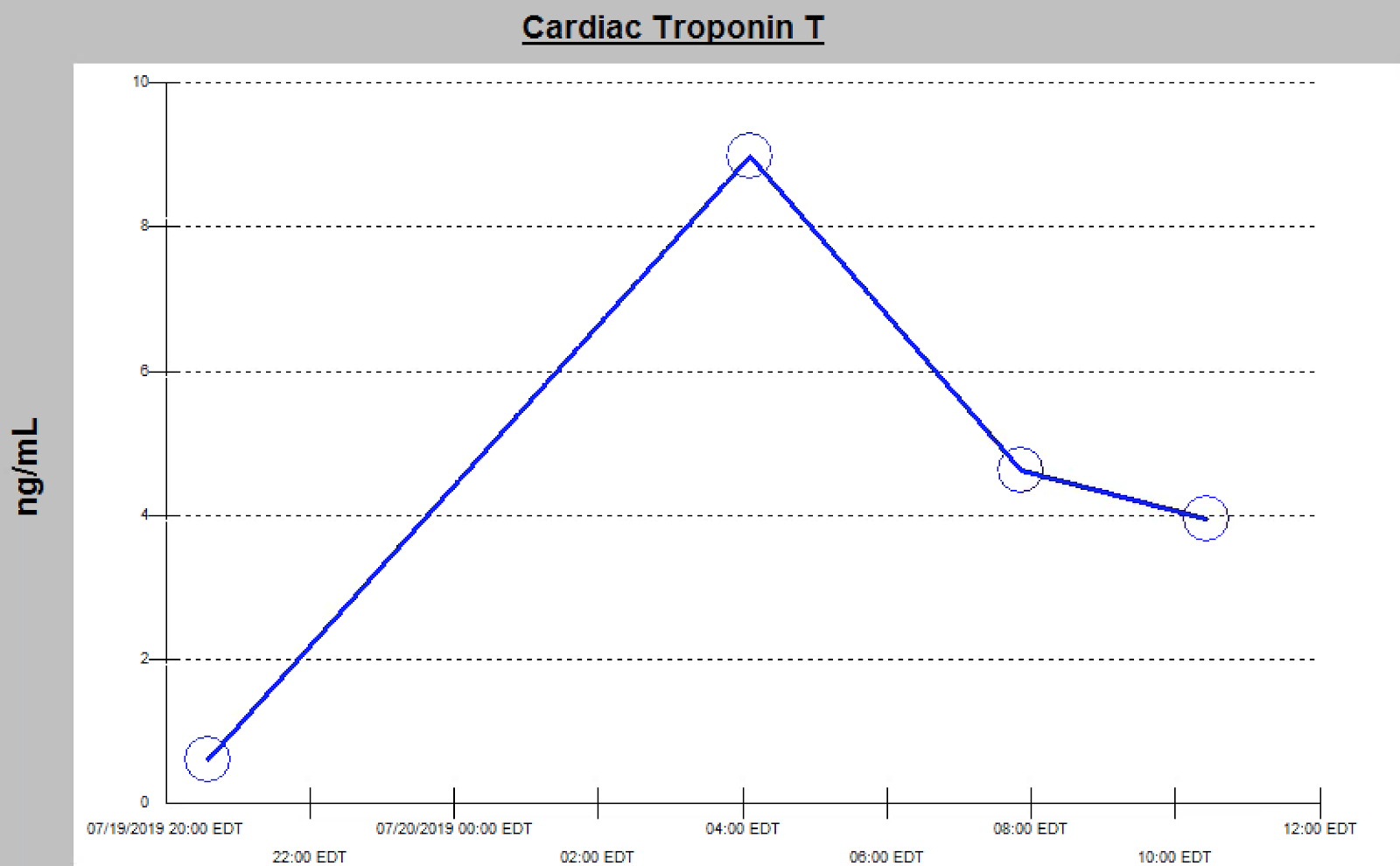
The initial troponin T returned at 0.61 ng/mL.
5.5 hours later a repeat troponin T was 9.0 ng/mL, consistent with very large myocardial infarction.
At the 24 hour mark a formal echocardiogram was performed which revealed severe hypokinesis of the anterior wall, septum, and apex with an ejection fraction of 27%.
Teaching points:
You must learn to identify OMI so that you can advocate for your patients.
What is obvious to you may not be to your colleagues and consultants. Adjunctive tests such as point of care ultrasound to look for wall motion abnormalities may make the difference between an emergent or delayed cath lab activation (think of it as the FAST exam for ACS!). You should routinely perform these POC echos in order to practice identifying wall motion abnormalities. An easy exercise is to start by performing a POC echo on all STEMI activations where it is clear there is a wall motion abnormality; when there is STEMI, if you do not see a WMA, then you are missing it.
Although this ECG is completely diagnostic, there is utility in emergent echo looking for wall motion abnormalities in cases where the ECG is less diagnostic, or when the provider(s) do not recognize OMI on a diagnostic ECG. Only high quality contrast echo done by a trained echocardiographer and read by an expert can approach true rule-out of a wall motion abnormality. An echo of any lesser quality can of course be used, with the understanding that it is really only helpful if you find a wall motion abnormality, thereby increasing your suspicion of OMI and helping the decision to proceed with emergent cath.
Do not let POCUS convince you of absence of OMI if the ECG is diagnostic. An inadequate echo, or one read by a non-expert, can be false negative.
Do not let POCUS convince you of absence of OMI if the ECG is diagnostic. An inadequate echo, or one read by a non-expert, can be false negative.
Don't forget to obtain serial ECGs. Even if progression to STEMI is not seen, dynamic changes (e.g., development of reperfusion pattern) can help to expedite appropriate treatment.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.