
Here is the ED ECG of a 58 yo male whose chest pain is resolved:
Without any ECG from earlier when the patient had chest pain, this is nondiagnostic. With a negative troponin, the patient would be admitted for observation.
Let's go back to the beginning:
A 58 yo male with a h/o CABG developed on and off chest pain which became constant while playing golf.
911 was called. Here is his initial prehospital ECG at 1129:
The computer read ***Acute MI***. The cath lab was activated prehospital.
He received aspirin and Nitroglycerin, had relief of chest pain, and had this ECG recorded at 1136:
Did NTG cause this reperfusion? That can't be known. But had this second ECG been the first one recorded, there would be no indication for immediate reperfusion.
He arrived in the ED and had this ECG recorded at 1153:
Imagine if you did not have the prehospital ECGs. It would be tough to diagnose ACS, in spite of a very high risk situation.
He did develop chest pain again, and had this ECG recorded at 1206:
The initial troponin was normal. He was taken for immediate angiography, where a 99% 2nd diagonal (2nd major lateral branch off the LAD) lesion was found and opened.
The next AM he had a completely normal echocardiogram with EF of 65%. Peak troponin was 0.85 ng/ml. Here is his ECG the next AM.
Thus, the next day, the ECG was more sensitive than echo for MI. This is not unusual, but sometimes, due to a negative echo, cardiologists can be convinced (in spite of contrary evidence), that no MI occurred. I have heard expressions of high faith in the sensitivity of echo for ACS.
Learning points:
1. NTG may cause reperfusion
2. Record an ECG before NTG
3. Always look at prehospital ECGs
4. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal.
Here is an interesting abstract regarding NTG after the EKG:
Mahoney BD, Hildebrandt DA, Allegra P. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Prehospital Emergency Care 2008;15:105, Abstract 24.
Hypothesis. The decision to take a patient for emergent reperfusion therapy is largely determined by an ECG diagnostic for ST Elevation Myocardial Infarction (STEMI). Hildebrandt et al have proven that prehospital 12 Lead ECGs followed by an immediate call for reperfusion team mobilization reduce door to balloon times.We hypothesize that prehospital ECGs will normalize in some STEMI patients after nitroglycerin (NTG)therapy or due to spontaneous reperfusion. NTG therapy before an ECG, or the absence of a prehospital ECG capacity in some services may lead to missing the early diagnosis of STEMI thus delaying reperfusion therapy. Methods. A prospective analysis of consecutive adult patients presenting to an urban/suburban two paramedic ambulance service fromJuly 15, 2006, to August 15, 2007, who have diagnostic ECGs for STEMI. Paramedics managing a possible myocardial infarction patient were instructed to obtain rapidly an ECG prior to treatment with NTG. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team. A second ECG was done prior to arrival at the ED. The ECGs were later reviewed by emergency physicians and cardiologists who confirmed the presence of a diagnostic prehospital ECG and STEMI. Results. During the 13 month interval, 87 patients had an initial ECG that was diagnostic for STEMI. These patients received no NTG from the paramedics prior to obtaining the first ECG. An average of 16 minutes 42 seconds later, 3 patients had an ECG that was no longer diagnostic for STEMI and 3 had a partial normalization in their ECG that made diagnosis of STEMI more difficult. Conclusions. Prehospital ECGs diagnostic for STEMI can normalize or become nondiagnostic after NTG administration or due to spontaneous reperfusion or evolution. In the absence of a prehospital ECG, it is possible that 6 of 87 (7%) of STEMI patients in this study would have had reperfusion delayed due to a rapid change in their ECG. Limitations includenocontrol groupreceiving NTG prior to the first ECG.
 |
| There is sinus rhythm with a PAC (which has aberrant conduction -- RBBB). There is nondiagostic ST depression in V3 and nondiagnostic ST-T abnormalities in precordial leads. |
Let's go back to the beginning:
A 58 yo male with a h/o CABG developed on and off chest pain which became constant while playing golf.
911 was called. Here is his initial prehospital ECG at 1129:
 |
| There is sinus rhythm and clear posterolateral STEMI, with ST elevation in I and aVL and reciprocal ST depression in III and aVF. There is ST depression in right precordial leads diagnostic of posterior STEMI. |
He received aspirin and Nitroglycerin, had relief of chest pain, and had this ECG recorded at 1136:
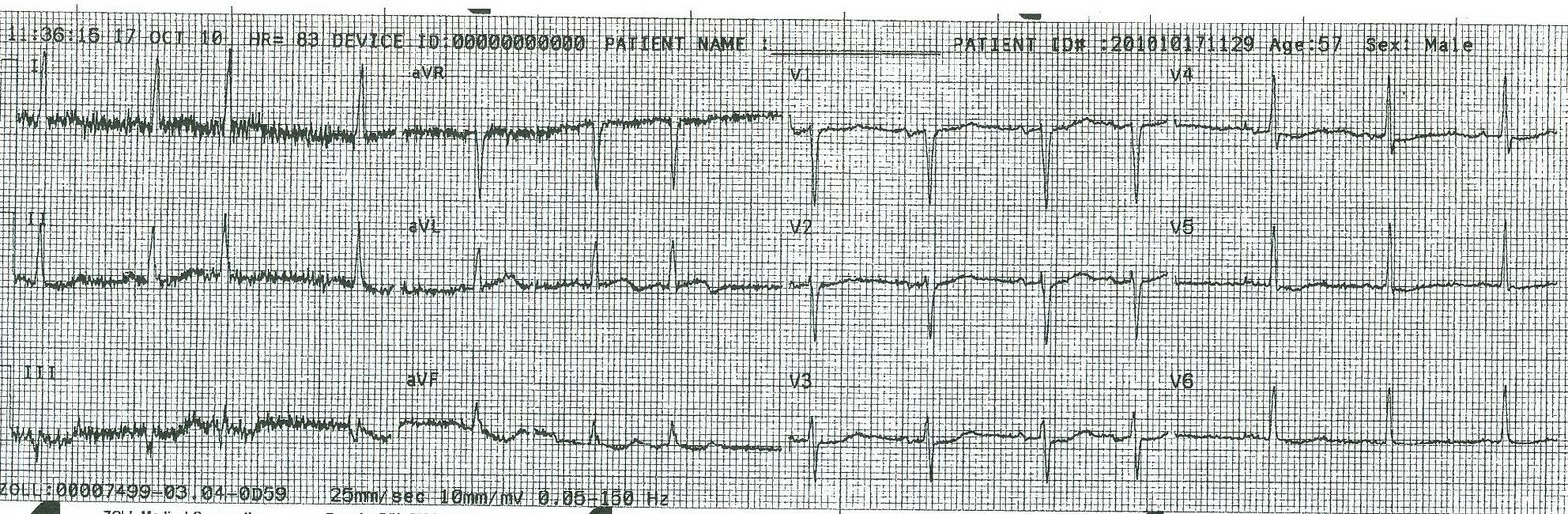 |
| There is now minimal ST elevation in aVL with minimal reciprocal ST depression. Clearly the artery is reperfused. |
He arrived in the ED and had this ECG recorded at 1153:
|
| This is the ECG shown first, above, with the PAC with aberrant RBBB conduction and non-diagnostic ST-T findings. |
He did develop chest pain again, and had this ECG recorded at 1206:
 |
| Sinus rhythm with 2 aberrantly conducted (RBBB) PACs. Now there is again ST elevation in aVL with reciprocal depression in lead III |
The initial troponin was normal. He was taken for immediate angiography, where a 99% 2nd diagonal (2nd major lateral branch off the LAD) lesion was found and opened.
The next AM he had a completely normal echocardiogram with EF of 65%. Peak troponin was 0.85 ng/ml. Here is his ECG the next AM.
 |
| Notice the reperfusion T-waves in I and aVL. |
Thus, the next day, the ECG was more sensitive than echo for MI. This is not unusual, but sometimes, due to a negative echo, cardiologists can be convinced (in spite of contrary evidence), that no MI occurred. I have heard expressions of high faith in the sensitivity of echo for ACS.
Learning points:
1. NTG may cause reperfusion
2. Record an ECG before NTG
3. Always look at prehospital ECGs
4. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal.
Here is an interesting abstract regarding NTG after the EKG:
Mahoney BD, Hildebrandt DA, Allegra P. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Prehospital Emergency Care 2008;15:105, Abstract 24.
Hypothesis. The decision to take a patient for emergent reperfusion therapy is largely determined by an ECG diagnostic for ST Elevation Myocardial Infarction (STEMI). Hildebrandt et al have proven that prehospital 12 Lead ECGs followed by an immediate call for reperfusion team mobilization reduce door to balloon times.We hypothesize that prehospital ECGs will normalize in some STEMI patients after nitroglycerin (NTG)therapy or due to spontaneous reperfusion. NTG therapy before an ECG, or the absence of a prehospital ECG capacity in some services may lead to missing the early diagnosis of STEMI thus delaying reperfusion therapy. Methods. A prospective analysis of consecutive adult patients presenting to an urban/suburban two paramedic ambulance service fromJuly 15, 2006, to August 15, 2007, who have diagnostic ECGs for STEMI. Paramedics managing a possible myocardial infarction patient were instructed to obtain rapidly an ECG prior to treatment with NTG. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team. A second ECG was done prior to arrival at the ED. The ECGs were later reviewed by emergency physicians and cardiologists who confirmed the presence of a diagnostic prehospital ECG and STEMI. Results. During the 13 month interval, 87 patients had an initial ECG that was diagnostic for STEMI. These patients received no NTG from the paramedics prior to obtaining the first ECG. An average of 16 minutes 42 seconds later, 3 patients had an ECG that was no longer diagnostic for STEMI and 3 had a partial normalization in their ECG that made diagnosis of STEMI more difficult. Conclusions. Prehospital ECGs diagnostic for STEMI can normalize or become nondiagnostic after NTG administration or due to spontaneous reperfusion or evolution. In the absence of a prehospital ECG, it is possible that 6 of 87 (7%) of STEMI patients in this study would have had reperfusion delayed due to a rapid change in their ECG. Limitations includenocontrol groupreceiving NTG prior to the first ECG.
Hello Dr. Smith,
ReplyDeleteI was curious about a few things. On the first ECG you said there was non-diagnostic STD in V3. I also see STD in V4 which would make me want to do a V7-V9 due to possible posterior MI.
The other one I noticed was the one done at 1206 which shows elevation in aVL and I with reciprocal changes in III and aVF. Correct me if I'm wrong please.
Dr. Smith,
ReplyDeleteAre you aware of any studies where NTG was given under flouroscopy and the resultant changes in the ECG recorded?
I've found studies of IV NTG drips under flouroscopy which noted increases in lumen diameter ~8% and decreases in plaque area around 4%. It makes sense that if its a near occlusion NTG could provide enough flow to normalize the ECG.
Yes, a posterior EKG might prove useful. As for the second question, it seems to be exactly what I wrote, or am I misunderstanding?
ReplyDeleteI am not aware of such studies. Any references are welcome. There is one old study (1980's) from England where they had very long prehospital times, and in which the ECG was done prehospital. If there was STEMI, the patients were given ASA and nitroglycerine and when they arrived at the hospital much later, 25% had reperfusion. I can't find the reference now.
ReplyDelete"Did NTG cause this reperfusion? That can't be known. But had this second ECG been the first one recorded, there would be no indication for immediate reperfusion."
ReplyDeleteIn that case should we also be recording ecgs before giving aspirin?
Good question. I would say yes.
ReplyDeleteAnd if spontaneous reperfusion(or aspirin/nitro assisted reperfusion) occurs, why is it so important to rush for reperfusion therapy?
ReplyDeleteBecause the reperfusion is provisional, tentative, and ready to close off at any moment.
ReplyDeleteDr smith if we don't have a cath lab can we give thrombolytic agents and if your answer is yed how to differentiate it from prinzmetal angina ?
ReplyDeleteif we don't have a cath lab can we give thrombolytic agents ?
ReplyDeleteif yes how to differentiate from prinzmetal angina ?
Prinzmetal's angina is very rare. Most of what historically was diagnosed as Prinzmetal's angina was thrombosis with autolysis of thrombus. That pathophysiology was not recognized for many years and took many years for it to be widely known. So forget Prinzmetal's unless there is a history of provocation of spasm during angiography.
Delete