
Case sent by Logan Stark MD, written by Pendell Meyers
A woman in her 70s presented with acute chest pain. It started 10 hours prior to arrival, then had improved, then recently returned. No prior ECG was available.
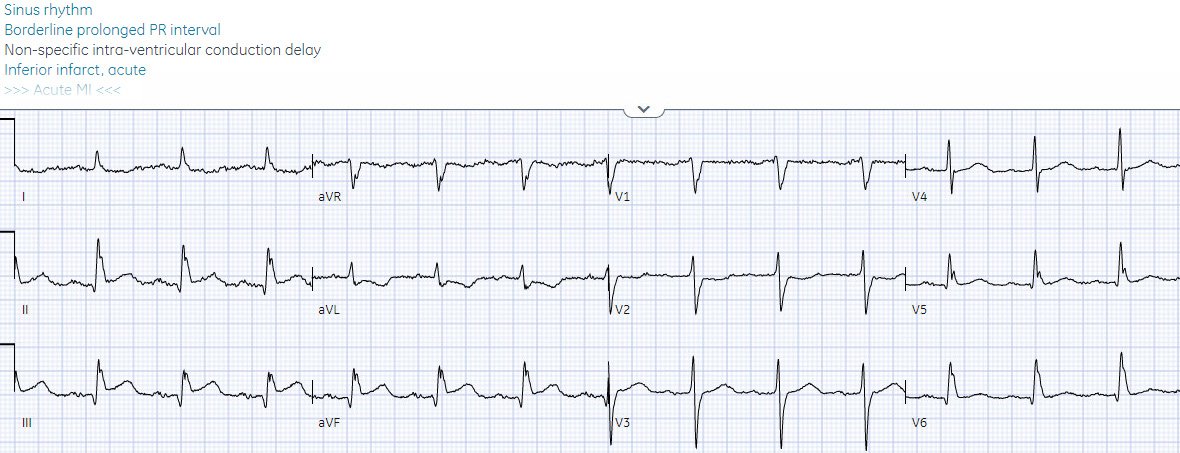
Here is her triage ECG:
 |
| What do you think? |
The ECG was sent to me with no information, and I replied "OMI".
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict:


V1 and V2 have abnormal STE, and V2 has a hyperacute T wave. There is reciprocal STD in II, III, and aVF.
One more thing that should be mentioned: since there are only Q waves from V1 to V3, it is possible that there was an old anterior wall MI, or that the current event is subacute, or acute on top of an old Q wave. Regardless, V2 with a hyperacute T wave and abnormal T/S ratio means there must be acute OMI, regardless of prior events. The pattern overall is similar to the "South African flag sign".
The initial high sensitivity troponin I returned at only 19 ng/L (which is elevated in this assay, as the URL is 12 ng/L for women). Does that change your interpretation??
NO!
Hopefully it confers even more benefit to reperfusion, since the troponin has not risen very high yet. Notice how the patients onset of symptoms (10 hours ago) is potentially misleading if you ignore the intermittent nature of her symptoms.
The cath lab was activated immediately (before the troponin of course), and the patient was taken to cath and found to have acute proximal LAD occlusion (unknown initial TIMI flow, but corrected to TIMI 3 with PCI).
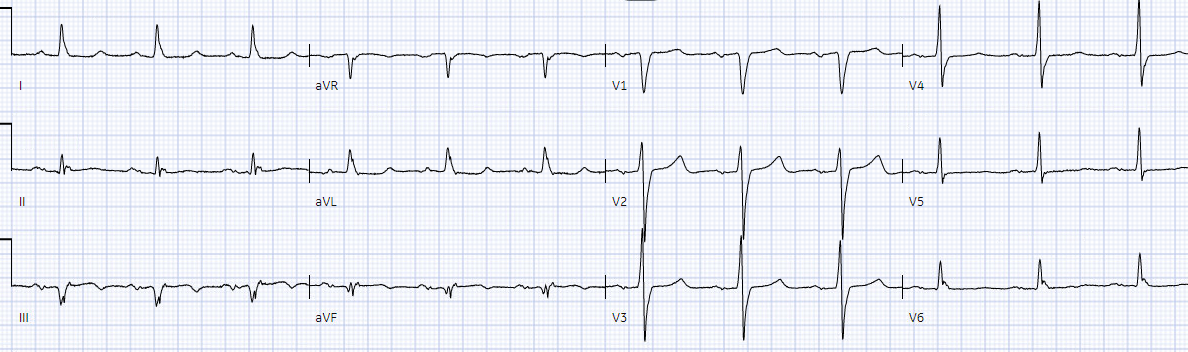
Here are her ECGs after cath over the next 12 hours:


YOU TOO CAN HAVE THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
===================================
MY Comment, by KEN GRAUER, MD (8/30/2023):
===================================
The 2 Key Questions regarding today’s presentation are the following:
- Question #1: Is the ECG in Figure-1 likely to represent an ongoing or recent OMI in need of prompt cath and PCI?
- Question #2: How fast can we answer Question #1?
For clarity in Figure-1 — I’ve reproduced the initial tracing in today’s case.
-USE.png) |
| Figure-1: The initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
Addressing the 2 KEY Questions:
For followers of Dr. Smith’s ECG Blog — it will often be easy and quick to answer these 2 Questions:
- Point #1: Is the history worrisome? Obviously a history of new-onset CP (Chest Pain) in a patient of a certain age and risk profile would immediately place the patient in a “higher-risk” group. Today's case involves a woman in her 70s who describes "acute CP" that began ~10 hours earlier — so this history clearly increases our concern.
- Point #2: Followers of Dr. Smith's ECG Blog who have long ago replaced the outdated "STEMI paradigm" with the much more sensitive and specific OMI Paradigm (most recently reviewed in Dr. Smith's OMI Lecture — and in Dr. Mark Hellerman's OMI Pocket Guide) — will immediately recognize the other critical piece of information in the history from today's patient = The patient's CP improved — and then returned, at which time she presented to the ED.
- The OMI Paradigm integrates the clinical reality that acute coronary occlusion may be punctuated by periods during which CP decreases as a result of spontaneous reopening of the "culprit" vessel — but that such spontaneous reopening may be followed at any point by spontaneous reclosure, sometimes with the "culprit" vessel spontaneously opening and closing a number of times until a final state is reached.
- As a result, marked ST elevation that may have been present at the onset of symptoms — may be greatly reduced (or even "pseudo"-normalized) — IF the initial ECG is obtained after a reduction of symptoms!
- Point #3: Ideally — We would have more information regarding the specifics correlating the timing and relative severity of this patient's symptoms — with the timing of when ECG #1 was obtained (ie, Had this patient's CP returned minutes — or an hour or more, before this initial ED ECG was recorded?).
- That said, even without that information — the history provided above by today's patient is potentially consistent with such spontaneous reopening of the "culprit" vessel — which means that despite a lack (or a minimal amount) of frank ST elevation — in this higher-risk patient with a very worrisome history for a recent or ongoing acute coronary event — even subtle signs of OMI suffice to warrant prompt cardiac catheterization!
What About Today's ECG?
Given the above history in today's case — I viewed ECG #1 asking myself, "Are there any ECG findings that are definitely abnormal enough to merit prompt cath?" While completely agreeing with Dr. Meyers' interpretation and the High-Confidence OMI interpretation by QOH (Queen Of Hearts) — I'll add the following perspective:
- As per Dr. Meyers — there are QS complexes in leads V1,V2,V3 (as well as an r wave that is still of small amplitude in lead V4). This lack of anterior forces could be an acute finding — and/or — indicative of an acute event superimposed on prior anteroseptal infarction.
- As per Dr. Meyers — the ST-T wave in lead V2 looks hyperacute (definite straightening of the ST segment takeoff in this lead — with a disproportionate amount of ST elevation given tiny size of the QRS — with a wider-than-expected ST segment base). But as potentially ominous as the ST-T wave in lead V2 looks — I wanted more evidence before concluding that ECG #1 represented definite indication for prompt cath.
- The ST segment in lead V1 is coved, with slight elevation and surprisingly deep T wave inversion — so clearly suspicious in association with lead V2 findings of proximal LAD occlusion — but I still wanted a bit more.
- Unfortunately — lead V3 is uninterpretable for assessing acute changes because of artifactual distortion of the ST-T wave in this lead. IF I were to still be in doubt about my interpretation after looking at all 12 leads — then the uninterpretable nature of this very important neighboring lead V3 could justify immediately repeating the ECG.
That said — Repeating ECG #1 was not necessary ...
- There is simply NO way that the ST-T waves in each of the inferior leads is a "normal" finding. Note that each of the ST segments in leads II,III,aVF are abnormally straight, slightly depressed — and finish with a disproportionately tall terminal T wave. Whether this is all a reflection of reciprocal changes to acute LAD OMI, or perhaps reflects some component of reperfusion change in this patient with waxing and waning CP, is uncertain. What is certain — is that these inferior lead ST-T wave changes + the hyperacute ST-T wave in lead V2 + the history in this 70s woman are diagnostic of recent and/or ongoing acute LAD OMI in need of prompt cath.
- Additional Findings in ECG #1: Completing my survey of all 12 leads in today's initial tracing — there is: i) A surprisingly unimpressive ST-T wave in lead aVL (I suspect that some of the ST elevation that usually accompanies acute proximal LAD OMI has "pseudo"-normalized because of a component of spontaneous reperfusion); ii) The T wave in lead V4 (and to a lesser extent — probably also the T waves in leads V5,V6) is also probably hyperacute (ie, disproportionately hypervoluminous compared to the small size of the QRS); and, iii) I suspect that if the artifact in lead V3 was eliminated — that the ST-T wave in this lead would manifest a "transition" appearance between the hyperacute T wave with ST elevation in lead V2 — and the non-elevated but hyperacute T wave in lead V4.
- BOTTOM Line: The decision that prompt cath is needed in today's case is one that can (should) be reached within the very few minutes needed to establish the history of waxing and waning CP over the previous 10 hours — and the minute or two that it takes to record this 1st ECG. Experienced providers versed in the OMI paradigm will recognize the above ECG changes I describe in less than 1 minute.
=======================================
ADDENDUM: What is the Rhythm in ECG #3 ???
=======================================
Did YOU notice that the 3rd ECG shown above in today's case has group beating? (ie, Alternating short-long R-R intervals for beats #1-2; 3-4; 5-6; 7-8; and 9-10 in Figure-2).
- As I've often emphasized in my comments in Dr. Smith's ECG Blog — the presence of group beating in association with an acute (or recent) MI should suggest the possibility of 2nd-degree AV Block, Mobitz Type I ( = AV Wenckebach). Is Mobitz I the cause of the group beating that we see in Figure-2?
-USE.png) |
| Figure-2: I've reproduced the 3rd ECG shown above by Dr. Meyers in today's case. Does the group beating that we see represent Mobitz I, 2nd-degree AV block? |
ANSWER:
Mobitz I, 2nd-degree AV block ( = AV Wenckebach) — is probably the most common AV conduction disturbance seen in association with acute or recent inferior MI. It is not nearly as common with acute LAD occlusion, as was seen on cath in today's case.
- The group beating seen in the long lead II rhythm strip of ECG #3 is unlikely to be the result of chance — since with the exception of the last 2 beats in the tracing, the shorter R-R intervals are of similar (albeit not exact) duration — and the longer R-R intervals are also of similar duration.
- We can definitely rule out 2nd-degree AV block of the Mobitz I type — because: i) The atrial rhythm is not regular; ii) The PR interval is not increasing from the 1st-to-the-2nd beat in each group; and, iii) There is no dropped (non-conducted) on-time P wave during the pauses, as there has to be with Mobitz I.
- The rhythm in Figure-2 is also not Mobitz II because: i) The QRS is not wide (as it usually is with Mobitz II); and, ii) There is no dropped (non-conducted) on-time P wave during the pauses, as there should be with Mobitz II.
- Although sinus arrhythmia may sometimes occur in a pattern that resembles "group beating" — I thought the difference in R-R interval duration between shorter and longer cycles in Figure-2 was much greater than would be expected with sinus arrhythmia.
This left 2 additional considerations. I've drawn laddergrams in Figure-3 and Figure-4 to illustrate these 2 remaining possibilities.
- As I emphasize in my September 26, 2020 post of Dr. Smith's ECG Blog — the most common cause of a pause is a blocked PAC (and not some form of AV block).
- IF the cause of the group beating that we see in ECG #3 is blocked PACs — then a laddergram of this would look like Figure-3, in which the early-occurring PACs would be hiding under the BLUE arrows. When PACs occur very early during the cycle — they may fall within the ARP (Absolute Refractory Period), and therefore not be conducted
- That said — I simply can not convince myself that there is any evidence of "tell-tale" notching indicative of a hidden PAC within any of the even-numbered beat T waves in any of the simultaneously-recorded leads seen in Figure-2.
-USE.png) |
| Figure-3: Laddergram showing what blocked PACs would look like. |
As I discuss in My Comment at the bottom of the page in the May 25, 2022 post in Dr. Smith's ECG Blog — SA Block is a potential cause of repetitive group beating in which the atrial rhythm is not regular — the PR interval does not increase — and the in which there is no non-conducted P wave within the longer R-R intervals.
- IF the cause of the group beating that we see in ECG #3 is SA block — then a laddergram of this might look like Figure-4, in which the rate of impulse formation from the SA node remains regular (with minimal variation due to sinus arrhythmia) — but only 2 out of every 3 SA nodal impulses are able to make it out of the SA node into the atria.
- That said — SA block is rare. I would simply not expect to see it in the very last ECG in today's case at a time when PCI successfully reestablished flow to the "culprit" artery, and the patient was otherwise doing well.
-USE.png) |
| Figure-4: Laddergram showing what SA block would look like. |
BOTTOM Line regarding the Rhythm in ECG #3:
I fully acknowledge not knowing the cause of the group beating that we see in ECG #3.
- Perhaps the most common cause of short pauses is operative — with blocked PACs being completely hidden within the T waves under the BLUE arrows in Figure-3?
- Or perhaps the group beating is simply the result of sinus arrhythmia that by chance results in alternating R-R intervals of very similar size?
- MY Hunch: I suspect that the cause of the group beating we see in ECG #3 is benign, whatever the specific etiology turns out to be. I wish a little longer period of monitoring would have been obtained — which I suspect would have told us what the true cause is. That said — the sharp clinician who does not want to overlook rhythm disorders will be systematic in the assessment of every rhythm encountered — and will not overlook the group beating present in today's 3rd ECG.
- P.S.: I'll close with this link to My Comment in the April 6, 2023 post in Dr. Smith's ECG Blog — in which I illustrate how failure to be systematic in rhythm assessment (with failure to recognize group beating) — resulted in overlooking an AV block that was clinically significant.



-USE%20copy.png)


-USE.png)