
This case was sent by Laszlo Farkas, a paramedic from Hungary. He discussed it with Janos Borbas MD and Robert Sepp MD from University of Szeged 2nd
Department of Internal Medicine and Cardiology Clinic.
The case inspired me to resurrect a case that I published 10 years ago with the same ECG finding (2nd case below).
What is the finding?
What does it signify?
Case
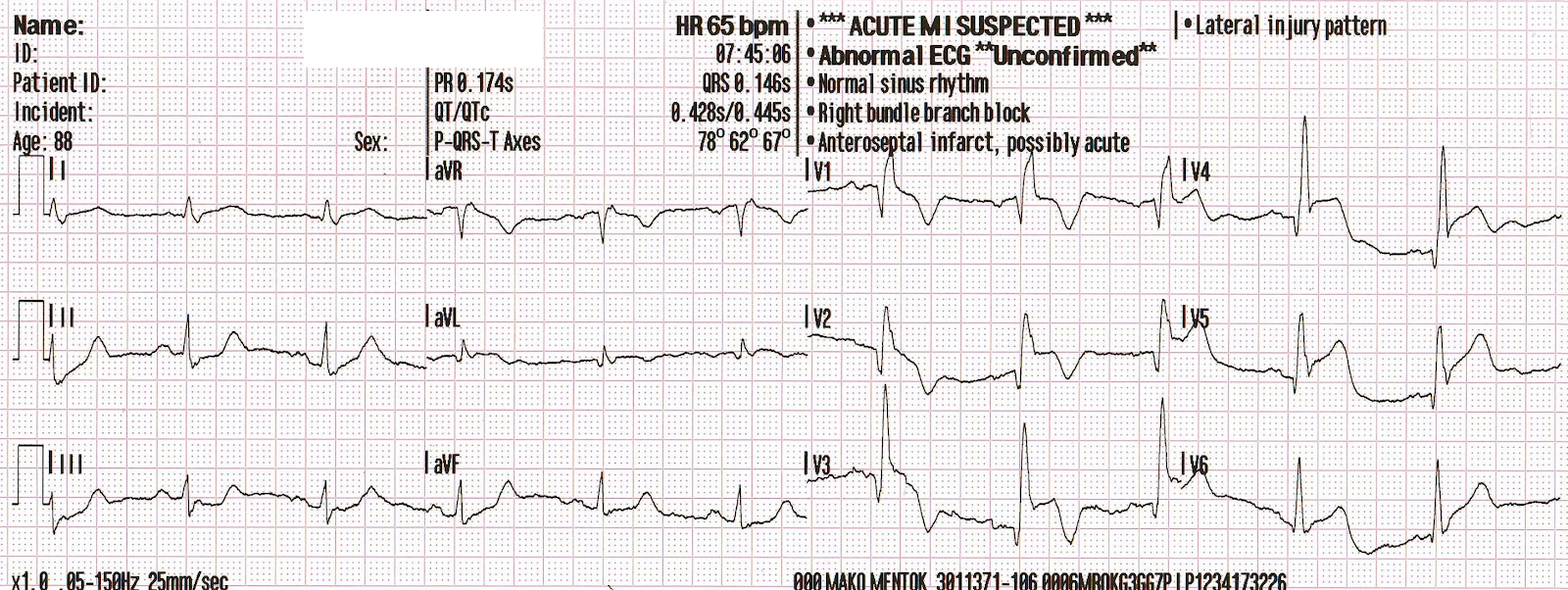
An elderly male presented with chest pain. Here is the first ED ECG:
This ECG that I published 10 years ago in Critical Decisions in Emergency and Acute Care Electrocardiography has the same finding:
The finding is an inverted U-wave, as demonstrated with arrows here:
Here is the ECG from Laszlo's case again:
In Laszlo's case, he recognized it and recorded another ECG 35 minutes later:
This is after reperfusion and stenting of an occluded LAD:
And then 13 minutes later:
Here is case 2:
This shows the initial ECG shown again, the comparison ECG from previous, and the reperfusion ECG after stenting of LAD that had severe subtotal thrombotic occlusion with TIMI-2 flow:
This 89 year old had an episode of unresponsiveness.

Previous ECG:

First ECG with arrows (again)
The case inspired me to resurrect a case that I published 10 years ago with the same ECG finding (2nd case below).
What is the finding?
What does it signify?
Case
An elderly male presented with chest pain. Here is the first ED ECG:
 |
| Hint: the finding is NOT the T-wave inversion in aVL |
This ECG that I published 10 years ago in Critical Decisions in Emergency and Acute Care Electrocardiography has the same finding:
 |
| What is the finding? |
The finding is an inverted U-wave, as demonstrated with arrows here:
 |
| Inverted U-waves in a patient with chest pain are reported to be highly specific, but insensitive, for ischemia/infarction. |
Here is the ECG from Laszlo's case again:
 |
| See the inverted U-waves in V3, V4, V5 |
In Laszlo's case, he recognized it and recorded another ECG 35 minutes later:
 |
| Now the U-waves are not the issue. There is obvious STEMI. |
This is after reperfusion and stenting of an occluded LAD:
 |
| Terminal T-wave inversion, consistent with reperfusion. |
And then 13 minutes later:
 |
| Resolution of much of the ST Elevation (but not all). Now U-waves are upright in V2-V550-70% reduction in STE is good evidence of tissue reperfusion (there can be reperfusion of the artery without reperfusion of the myocardium, called "No Reflow", and the ECG is the best predictor of reflow, correlating closely with angiographic "myocardial perfusion grade," or "blush") |
Here is case 2:
This shows the initial ECG shown again, the comparison ECG from previous, and the reperfusion ECG after stenting of LAD that had severe subtotal thrombotic occlusion with TIMI-2 flow:
This 89 year old had an episode of unresponsiveness.

Previous ECG:

First ECG with arrows (again)
 |
| Slight STD in inferior and lateral leads, some STE in aVL, and profound negative U-waves in V3-V5. |
After Reperfusion of LAD:
 |
| Reperfusion T-waves (Wellens' waves) |
Short
Summary of the U-wave
[Adapted
from one of my chapters (in the ACS section, which I edited) in Critical
Decisions in Emergency and Acute Care Electrocardiography. There are some
contributions by Farkas Laszlo.]
Note: The research on this
topic is not of the most robust quality as the finding is unusual, it is not a
common finding, and there is not a lot of angiographic ECG research on this.
A U-wave is a low
amplitude, usually positive monophasic deflection after the T-wave, usually
with the same vector as the T-wave. It is co-incident with Phase 4 of the
action potential. The exact etiology of the U wave remains
unclear. Hypotheses include repolorization of the Purkinje fibers and
Mechanical Rebound of the myocardium at the end of systole. It is normally
less than 2 mm in height AND less than 25% of the T-wave in height. U wave
duration is about 170+-30 ms. It is usually positive in II, isoelectric in aVL
and aVR and may be, less commonly, inverted in III and aVF. It
should be upright in precordial leads. When inverted in
the precordial leads, it implies structural or ischemic heart disease. It
is normally less than 2 mm in height AND less than 25% of the T-wave in height.
What
are the implications of negative U-waves?
A negative U-wave,
other than in lead aVR, III, or aVF, implies ischemic heart disease. It has
been described during variant (vasospastic) angina attacks and during
stress testing, under which circumstances it has shown high specificity (though
low sensitivity) for the presence of a significant LAD stenosis. It
may also be seen with uncontrolled hypertension, under which circumstances
the U wave is usually negative-positive (biphasic), whereas in acute ischemia
it is more likely to be positive-negative. In a patient with
acute chest pain, a negative U-wave in the precordial leads represents a
significant LAD lesion until proven otherwise. Interestingly,
patients with an anterior wall MI and negative U-waves in the precordial leads
have been reported to have smaller infarcts, less STE, better collateral
circulation, and a larger amount of stunned but viable myocardium, but the
numbers are small. Similarly, a prominent negative U-wave in all
inferior leads in the presence of chest pain may be due to inferior ischemia. This
negative U-wave may indeed, as with terminal T-wave inversion, signify
spontaneous reperfusion.
A Negative U wave may
also be found in patients with valvular heart disease, congenital heart
disease, hyperthyroidism, and cardiomyopathies.
What
are the implications of an increased amplitude positive U-wave in the
precordial leads?
Prominent U waves
(exceed 1 mm) can be seen in hypokalemia, early repolarization, bradycardia,
hypothermia, left ventricular enlargement, atrioventricular block, congenital
long qt syndrome, left circumflex myocardial infarction.
Usually, U wave has the same polarity as the T wave. According to earlier findings discordance between T and U and concordant negative T and U wave can also predict hypertension or myocardial ischaemia.
In
the appropriate clinical context, an increase in U-wave amplitude in the
precordial leads may raise suspicion of posterior ischemia (due to an RCA or
LCX lesion). This could be considered the mirror image of a negative
U-wave.
Here
is a very nice full text article on the U-wave:
References
1. Yamaguchi
H, Ishimura T, Nishiyama S, et al. Hypertrophic nonobstructive cardiomyopathy
with giant negative T waves (apical hypertrophy): ventriculographic and
echocardiographic features in 30 patients. Am J Cardiol 1979; 44:401-12.
2. Miwa
K, Murakami T, Kambara H, Kawai C. U wave inversion during attacks of variant
angina. Br Heart J 1983; 50:378-82.
3. Gerson
MC, Phillips JF, Morris SN, McHenry PL. Exercise-induced U-wave inversion as a
marker of stenosis of the left anterior descending coronary artery. Circulation
1979; 60:1014-20.
4. Gerson
MC, McHenry PL. Resting U wave inversion as a marker of stenosis of the left
anterior descending coronary artery. Am J Med 1980; 69:545-50.
5. Kishida
H, Cole JS, Surawicz B. Negative U wave: a highly specific but poorly
understood sign of heart disease. Am J Cardiol 1982; 49:2030-6.
6.Miwa
K, Miyagi Y, Fujita M, Fujiki A, Sasayama S. Transient terminal U wave
inversion as a more specific marker for myocardial ischemia. Am Heart J 1993;
125:981-6.
7. Tamura
A, Nagase K, Mikuriya Y, Nasu M. Relation between negative U waves in
precordial leads on the admission electrocardiogram and time course of left
ventricular wall motion in anterior wall acute myocardial infarction. Am J
Cardiol 1999; 84:332-4, A8.
8. Miyakoda
H, Endo A, Kato M, et al. Exercise-induced U-wave changes in patients with
coronary artery disease--correlation with tomographic thallium-201 myocardial
imaging. Jpn Circ J 1996; 60:641-51.
9. Chikamori
T, Takata J, Seo H, et al. Diagnostic significance of an exercise-induced prominent
U wave in acute myocardial infarction. Am J Cardiol 1996; 78:1277-81.
10. Girish
MP, Gupta MD, Mukhopadhyay S, Yusuf J, Sunil Roy TN, Trehan V. U wave: an
important noninvasive electrocardiographic diagnostic marker. Indian Pacing
Electrophysiol J. 2005 Jan 1;5(1):63-5. PMID: 16943944
11.
Sovari AA, Farokhi F, Kocheril AG. Inverted U wave, a specific electrocardiographic sign of
cardiac ischemia. Am J Emerg Med. 2007 Feb;25(2):235-7.
12.
Pérez Riera AR, Ferreira C, Filho CF, Ferreira M, Meneghini A, Uchida AH,
Schapachnik E, Dubner S, Zhang L. The enigmatic sixth wave of the
electrocardiogram: the U wave. Cardiol J. 2008;15(5):408-21. Review. PMID:
18810715
13. Borbás J, Hategan L, Környei L, Katona
M, Csányi B, Tringer Annamária, Forster T, Sepp R. Qualitative and
quantitative assessement of ECG characteristics in patients with Andersen-Tawil
syndrome. Scientific Congress of Hungarian Society of Cardiology - Cardiologia
Hungarica, 2016.
i've got enough trouble with the original five waves, Steve, without throwing in the enigmatic sixth.
ReplyDeletethat first ekg by Lazlo Farkas could easily have gotten by me (before tonight). although, aVL did look unhealthy with the inverted T, and very slight hint of ST elevation (?). and even V2 looks "ill" with a low amp QRS, slightly biphasic T, and ? poor R wave progression from V1 to V2 to V3, (or is that my imagination).
what's very frightening is Lazlo's next . i guess there was less need for discussion with the cath team then.
thank you, again
tom
Excellent points by Dr. Smith in this Blog post about recognition and clinical significance of U wave inversion. In my experience, U wave inversion is uncommon (if not rare) — though part of that might reflect how easy it is to overlook this finding! Dr. Smith highlights 2 superb cases of U wave inversion in this post! That said — I believe even without the marked U wave abnormalities seen here — that BOTH cases should be picked up by the presence of other findings. ECG #1 (the case by Laszlo Farkas) — Not only is the T wave abnormally inverted in lead aVL — but there is also a large Q in aVL, and a clearly abnormal coved ST segment in this lead. Some isolated T inversion may at times be normal in aVL — but usually this is when the QRS is predominantly negative in this lead, and in view of the tiny R wave amplitude seen here in aVL — the depth and width of the T inversion seen here is clearly abnormal. Confirmation in a patient with chest discomfort that these findings in aVL are acute is forthcoming from EACH of the 3 inferior leads, all of which show an inappropriately flat ST segment with abrupt angulation rising to a prominent (fatter-than-it-should-be) T wave — which in effect is the mirror-image ( = reciprocal change) of the ST-T wave that we see in lead aVL. This picture in a patient with chest pain to me suggests OMI-in-progress until proven otherwise. As for ECG #2 (Dr. Smith’s wonderful case from 10 years ago) — there is subtle-but-real ST flattening with slight depression in no less than 7 leads with subtle-but-real ST elevation in lead aVR. Assuming serum electrolytes are normal — this ECG picture in an older adult should suggest significant coronary disease until proven otherwise. THANKS again to Dr. Smith for publishing 2 superb examples of clinically important U wave inversion!
ReplyDeleteThank you dr.smith for the wonderful cases and the great insight of the importance of U waves in ischemia.
ReplyDeleteThanks to dr.grauer for further expert reading of these cases.