
This was sent by Jason Winter of the Facebook Page Clinical Electrocardiology
This post presents one new case, then reviews some interesting aspects of high lateral MI and of ST Depression in "inferior" leads. Down below are 3 more cases and a discussion of how to differentiate false positive isolated STE in aVL from True positive.
Case
A 47 year old male called 911 for severe chest pain. He was clammy and looked unwell. He had a previous MI with cardiac arrest 2 years prior.
This is his prehospital ECG:
 |
| There is very subtle ST elevation in I and aVL, with very subtle ST depression in III and aVF. Is this due to coronary occlusion? |

Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer:
This is a posterolateral MI. Probably due to occlusion of the circumflex or one of its obtuse marginal branches.
Why did I say this?
1. The inferior ST depression is reciprocal to high lateral subtle STE
2. There is a down-up T-wave in aVF. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL.
3. ST segment in V2 has minimal ST elevation and is very flat, and the one in V3 is actually subtly downsloping. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. Together they strongly suggest a circumflex lesion.
The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion.
Later, the patient was taken to the cath lab. The artery was occluded. It was opened and stented. I could not get details on which artery, but I'm sure it was the circumflex.
Important Learning Point:
"STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion.
"Inferior" ST Segment Depression
It is important to understand that "inferior" ST Depression is not due inferior wall ischemia. Data from stress testing proves that the ST depression of ischemia does not localize. See this article:
Relation between the electrocardiographic stress test and degree and location of myocardial ischemia
When there is ischemic ST depression localized to the "inferior" leads, it is more likely to be reciprocal to ST elevation that localizes to the high lateral wall (aVL), even though that ST elevation may be nearly invisible. The ST depression may be the most visibly obvious sign of STEMI.Here is a case that demonstrates this very well:
Isolated "Inferior" ST Segment Depression: Not a Sign of Inferior Ischemia
Here is the most viewed post of all time on Dr. Smith's ECG Blog, with nearly 100,000 views:
Five Primary Patterns of Ischemic ST depression, without ST elevation. Some are STEMI-equivalents.
True Positive ST elevation in aVL vs. False Positive ST elevation in aVL
Case 1.
A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chest pain with radiation to the anterior neck, with associated nausea. She had known HTN and DM. She appeared to be in distress. She was given sublingual NTG with improvement, but there was not complete resolution.
Here was here initial ECG:
There was an old ECG for comparison:
A bedside cardiac ultrasound was done by the emergency physician. Here is the parasternal short axis view:
There is an anterior and lateral wall motion abnormality.
This still helps to show the wall motion abnormality:
The Cath Lab was activated, and here are the results:
1. LM: No significant stenosis.
2. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis. (Culprit, stented)
3. LCX: Luminal irregularities, no significant stenosis. Two OM branches without significant stenosis.
4. RCA: dominant. Luminal irregularities without significant stenosis. Supplies a small RPDA and RPLA.
This was the post-cath ECG:
A large Diagonal artery may supply both the lateral wall and part of the anterior wall.
He was given aspirin, clopidogrel, IV nitroglycerine, and heparin, the general cardiologist was called and notified that this patient was very high risk and needed close attention. He readily agreed, and the plan was to admit for close observation, serial ECGs and troponins, and to scrutinize for any recurrence of pain or change in the ECG.
The first troponin I then returned at 0.063 ng/ml (upper limit of normal = 0.025 ng/ml). Repeat ECG remained unchanged.
--He remained pain free and the plan remained to admit with a diagnosis of Non-STEMI on medical therapy with plan for angiogram in the morning.
--Just before admission to the hospital, the patient admitted to recurrent pain and appeared uncomfortable. Therefore, the cath lab was activated urgently.
--The suspicion was for a circumflex (or obtuse marginal branch) or diagonal artery occlusion or subtotal occlusion.
--At cath, there was a 95% proximal LAD stenosis with TIMI-II flow, proximal to a large diagonal. A stent was placed and the patient became pain free.
Lessons:
When there is ST elevation in aVL, with reciprocal ST depression in III:
1. Look for:
a. J-waves
b. Other ST depression
c. Large T-waves
d. Symmetric T-waves
e. Down-Up T-waves
2. Compare with an old ECG
3. Use ED Echo if available
4. Use formal Echo
5. A positive troponin is helpful (a negative one is not)
6. Angiogram if necessary. You don't want to miss an occlusion.
A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chest pain with radiation to the anterior neck, with associated nausea. She had known HTN and DM. She appeared to be in distress. She was given sublingual NTG with improvement, but there was not complete resolution.
Here was here initial ECG:
 |
| There is ST elevation in I and aVL, with inferior reciprocal ST depression in all of II, III, and aVF, and a down-up T-wave in aVF (a sign that is very specific for ischemia). There is also ST depression in V3-V6. This ECG is diagnostic of ischemia. |
It is important to compare this one with the false positive case #3 at the bottom; that one is a case which could fool you.
There was an old ECG for comparison:
 |
| One year prior with no ST segment abnormalities |
A bedside cardiac ultrasound was done by the emergency physician. Here is the parasternal short axis view:
There is an anterior and lateral wall motion abnormality.
This still helps to show the wall motion abnormality:
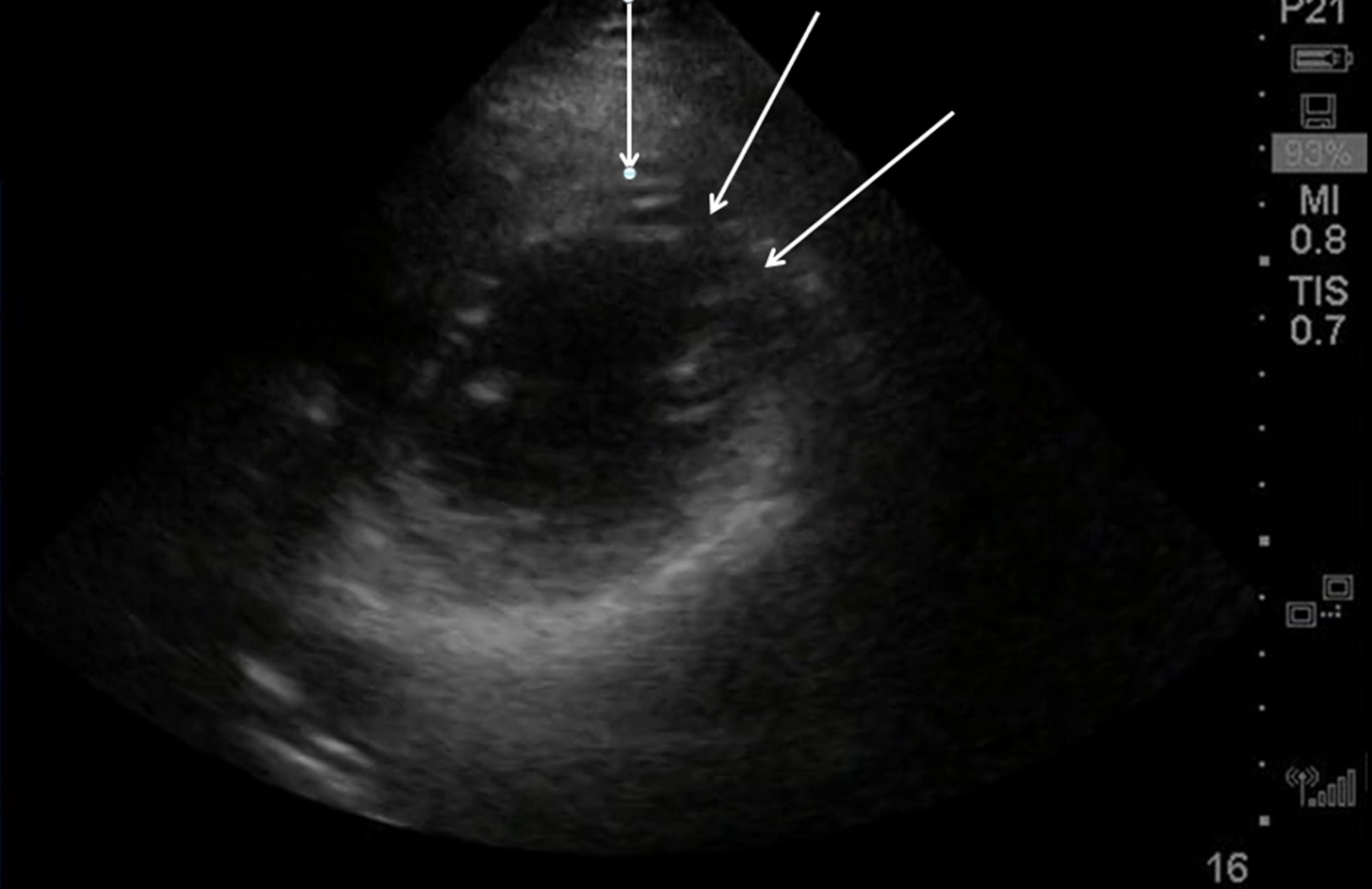 |
| Arrows point to area of wall motion abnormality |
The Cath Lab was activated, and here are the results:
1. LM: No significant stenosis.
2. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis. (Culprit, stented)
3. LCX: Luminal irregularities, no significant stenosis. Two OM branches without significant stenosis.
4. RCA: dominant. Luminal irregularities without significant stenosis. Supplies a small RPDA and RPLA.
After cath lab activation, her initial troponin returned at 0.124 ng/mL (99% level = 0.030 ng/mL)
 |
| After reperfusion: aVL shows resolution of ST elevation and inverted (reperfusion) T-wave. There is also some terminal T-wave inversion in anterior precordial leads |
A large Diagonal artery may supply both the lateral wall and part of the anterior wall.
Case 2: Another subtle lateral MI, from this post:
A male in his 60's presented 30 minutes after the onset of crushing substernal chest pain. Medics recorded 2 ECGs, one before and one after sublingual NTG, and both are similar to the first ED ECG. The patient had never had pain like this before. The pain improved from 9/10 to 3/10 after NTG. Here is the initial ED ECG:
 |
| There is subtle ST elevation in I and aVL with subtle reciprocal ST depression in III. Look at aVF. There is a downsloping reciprocal ST segement followed by an upright T-wave ("down-up" T-wave). This morphology is highly suspicious for ischemia. There are also symmetric anterior T-waves with very poor R-wave progression. T-waves in V4-V6 are taller than normal (compare to ECG in case 3 below) |
This ECG, especially along with the very typical
history, was very worrisome, but not absolutely diagnostic of, ischemia.
Several serial ECGs showed no change, even after the pain finally resolved to
0/10 after NTG.
He was given aspirin, clopidogrel, IV nitroglycerine, and heparin, the general cardiologist was called and notified that this patient was very high risk and needed close attention. He readily agreed, and the plan was to admit for close observation, serial ECGs and troponins, and to scrutinize for any recurrence of pain or change in the ECG.
The first troponin I then returned at 0.063 ng/ml (upper limit of normal = 0.025 ng/ml). Repeat ECG remained unchanged.
--He remained pain free and the plan remained to admit with a diagnosis of Non-STEMI on medical therapy with plan for angiogram in the morning.
--Just before admission to the hospital, the patient admitted to recurrent pain and appeared uncomfortable. Therefore, the cath lab was activated urgently.
--The suspicion was for a circumflex (or obtuse marginal branch) or diagonal artery occlusion or subtotal occlusion.
--At cath, there was a 95% proximal LAD stenosis with TIMI-II flow, proximal to a large diagonal. A stent was placed and the patient became pain free.
Case 3: False positive
And here is a similar one that is NOT MI. How do we tell the difference?
 |
| There is ST elevation in I and aVL, with reciprocal ST depression in lead III. |
Just so you don't think I'm cheating by using a retrospectoscope, this was sent to me without any outcome, and I read it as "no MI" with a high degree of certainty. This is because:
1. The remainder of the ECG is normal. No poor R-wave progression, no other ST depression, no symmetrical T-waves, no large T-waves, no down-up T-waves, typical early repol in anterior leads
2. The reciprocal ST depression is in lead III only. Not in leads II and aVF.
3. There are distinct J-waves in the two leads with ST elevation. This is highly suggestive of early repolarization in these leads.
4. The T-waves in I and aVL are not large (this was also true with the MI case 1 at the top, but that case had many other suspicious findings (many leads with ST depression and no J-waves)
5. There is ST elevation in V2-V4 that is clearly due to early repol. Early repol in aVL should be accompanied by early repol in the "anterior" leads.
When there is ST elevation in aVL, with reciprocal ST depression in III:
1. Look for:
a. J-waves
b. Other ST depression
c. Large T-waves
d. Symmetric T-waves
e. Down-Up T-waves
2. Compare with an old ECG
3. Use ED Echo if available
4. Use formal Echo
5. A positive troponin is helpful (a negative one is not)
6. Angiogram if necessary. You don't want to miss an occlusion.



GREAT post! Dr. Smith thoroughly covers all essentials in this case. A few quick thoughts I’d add are: i) Shape is much more important than amount of ST segment deviation. The shape of the ST-T wave in the original ECG presented in this case is clearly abnormal in multiple leads (the subtle-but real ST elevation in leads I,aVL; reciprocal ST-T wave changes in leads III,aVF; and either flat ST segment and/or abrupt angulation in the area of transition between ST segment and T wave in leads II and all 6 chest leads). Other than perhaps aVR — there are no truly normal leads here.
ReplyDeleteii) Think “mirror image” when looking for reciprocal changes. If you imagined a horizontal mirror running across the tracing in between lead III and lead aVL — then flipping lead III up would give you the picture we see in aVL, and vice versa.
iii) Dr. Smith’s pearl about the “down-up” T wave in lead aVF (subtle as it is) — is truly telling (ie, confirmatory).
THANKS for posting this case!