
There are many interesting facets to this case. I have highlighted the clinical factors over the ECGs, but the ECGs are very instructive as well: even after successful PCI with good (TIMI-3) in the epicardial coronary artery, there are ECG signs of poor microvascular perfusion, often called "No Reflow."
Case
A 31 year old male. No known past medical history. No cardiac risk factors.
Here is a great medical student history:
The patient presents to the ED with a complaint (through an interpreter) of a sore and itchy throat which led to feelings of generalized body pains that the patient describes as "cold pains" and feeling "tense/revved-up" or anxious and like he needed to "leave the room to scream, yell, and run around". The throat pain is described as sore, tight, itchy and it resolved with the ending of each "episode," each of which lasted ~5-10 minutes and completely resolved. Similar episodes continued to recur throughout the day and would last ~5-10 minutes and resolve with periods of feeling normal in between each one.
He endorses similar episodes one time 3 months ago and 1 week ago.
He exercises regularly without exertional CP or dyspnea. He denies Chest Pain or tightness, palpitations, SOB, vision changes, diaphoresis, dizziness, or voice changes. He had an episode while in ED that included his usual symptoms + HA, mild epigastric discomfort (consistent with his previous "gastritis pain") and nausea.
The faculty physician asked several times about chest pain or SOB and the answer was consistently "no."
Physical Exam: normal except that the patient had one episode while in the ED and had appeared anxious and kept changing positions.
Here is the ED ECG:
31 minutes later, while awaiting angiography, this was recorded:
He was taken for angiography. A 95% thrombotic occlusion (with TIMI-2 flow, consistent with the second ECG) of a type III (wraparound to inferior wall) LAD was found. It was occluded proximal to the first diagonal to the lateral wall. It was opened. There was much downstream showering of thrombi, some of which could be suctioned out.
Here is the post cath ECG:
Here is the next day ECG:
The first troponin I was 2.3 ng/mL and the 4th was 95.3 ng/mL (very high). No peak was measured. The echo showed anterior, apical, and inferior wall motion abnormalities.
This large possibly deadly STEMI could easily have been missed if the emergency physician was not attuned to the possibility of MI in patients with nonspecific symptoms. ECGs are cheap and noninvasive.
The only problem with recording ECGs on such patients is not that the vast majority will be normal (they will be), but that many will have non-diagnostic findings such as non-diagnostic T-wave inversion. One must learn which of the many nondiagnostic ECG patterns are truly worrisome.
Mostly, in patients at very low risk and with very nonspecific symptoms, we are looking for the unequivocally diagnostic ECG. When it is unequivocal, as in this case, it does not matter what the symptoms are: act on it.
Young patients: Young patients do have STEMI much more than is commonly recognized. I have presented many including these two 20-somethings here and here. When the cardiologist was called, the physician said, "OK, this is not straightforward, but hear me out." The cardiologist said "How old is the patient?" The answer was: "Thirty-one" and the cardiologist said, "Then it's not a STEMI."
Case
A 31 year old male. No known past medical history. No cardiac risk factors.
Here is a great medical student history:
The patient presents to the ED with a complaint (through an interpreter) of a sore and itchy throat which led to feelings of generalized body pains that the patient describes as "cold pains" and feeling "tense/revved-up" or anxious and like he needed to "leave the room to scream, yell, and run around". The throat pain is described as sore, tight, itchy and it resolved with the ending of each "episode," each of which lasted ~5-10 minutes and completely resolved. Similar episodes continued to recur throughout the day and would last ~5-10 minutes and resolve with periods of feeling normal in between each one.
He endorses similar episodes one time 3 months ago and 1 week ago.
He exercises regularly without exertional CP or dyspnea. He denies Chest Pain or tightness, palpitations, SOB, vision changes, diaphoresis, dizziness, or voice changes. He had an episode while in ED that included his usual symptoms + HA, mild epigastric discomfort (consistent with his previous "gastritis pain") and nausea.
The faculty physician asked several times about chest pain or SOB and the answer was consistently "no."
Physical Exam: normal except that the patient had one episode while in the ED and had appeared anxious and kept changing positions.
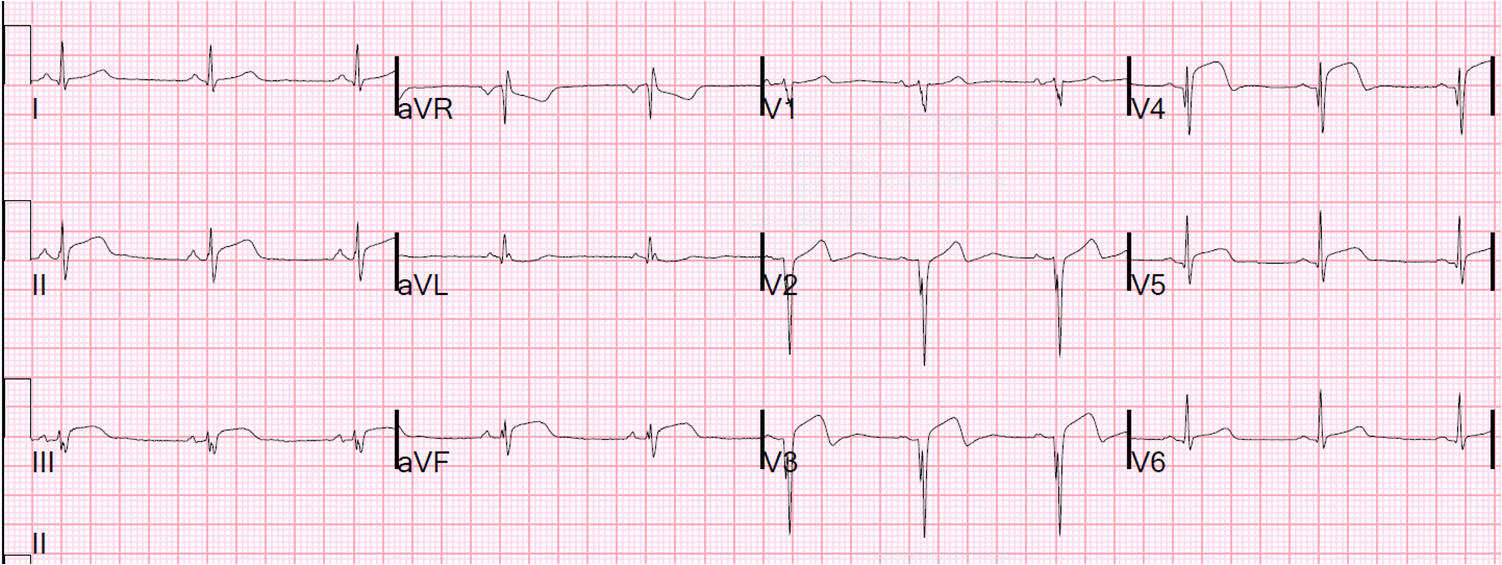
Here is the ED ECG:
 |
| There is sinus rhythm. There are anterior Q-waves, suggestive of previous infarction or prolonged infarction. Inferior ST elevation diagnostic of inferior STEMI. Convex ST elevation in V3 and V4 diagnostic of anterior STEMI. STE in V5 and V6 diagnostic of lateral STEMI. ST depression in V2 and V3 are suggestive of posterior involvement vs. de Winter's T-waves. |
31 minutes later, while awaiting angiography, this was recorded:
 |
| The T-waves are inverting in V2-V4, suggesting that the artery is open now. |
He was taken for angiography. A 95% thrombotic occlusion (with TIMI-2 flow, consistent with the second ECG) of a type III (wraparound to inferior wall) LAD was found. It was occluded proximal to the first diagonal to the lateral wall. It was opened. There was much downstream showering of thrombi, some of which could be suctioned out.
Here is the post cath ECG:
 |
| There
is persistent ST elevation. There is less than 50%, and even less than
70%, resolution of ST elevation. This is a bad prognostic sign and
suggests diffuse microvascular occlusion with persistent ischemia (No Reflow). There is a high risk of development of LV aneurysm when the ST elevation does not resolve, especially when there are Q-waves already. |
 |
| ST elevation remains persistent. No resolution of Q-waves. |
The first troponin I was 2.3 ng/mL and the 4th was 95.3 ng/mL (very high). No peak was measured. The echo showed anterior, apical, and inferior wall motion abnormalities.
This large possibly deadly STEMI could easily have been missed if the emergency physician was not attuned to the possibility of MI in patients with nonspecific symptoms. ECGs are cheap and noninvasive.
The only problem with recording ECGs on such patients is not that the vast majority will be normal (they will be), but that many will have non-diagnostic findings such as non-diagnostic T-wave inversion. One must learn which of the many nondiagnostic ECG patterns are truly worrisome.
Mostly, in patients at very low risk and with very nonspecific symptoms, we are looking for the unequivocally diagnostic ECG. When it is unequivocal, as in this case, it does not matter what the symptoms are: act on it.
Young patients: Young patients do have STEMI much more than is commonly recognized. I have presented many including these two 20-somethings here and here. When the cardiologist was called, the physician said, "OK, this is not straightforward, but hear me out." The cardiologist said "How old is the patient?" The answer was: "Thirty-one" and the cardiologist said, "Then it's not a STEMI."
Here are a number of cases in young women.
To his credit, he relented when he saw the ECG.
Door to EKG time: the door to EKG time was 3 hours in this case. But it is a miracle that any ECG was recorded. Management of this case was exemplary because any ECG was recorded. However, because it was recorded, it was recorded late, and thus the door to balloon time was long. This sort of management could harm your statistics even though it helps your patient. Institutions where a patient like this would not get an ECG would protect their DBT averages!!
STEMI patients without chest pain: In spite of a clear absence of chest pain or SOB on history done prior to the ECG, there were many mentions on the inpatient chart of the patient having had "chest discomfort" and "shortness of breath". It is very common for physicians to impute chest discomfort after seeing a STEMI on the ECG. They cannot imagine that someone can have a STEMI without any chest discomfort, or at least SOB. But this does happen. See this case in which, after seeing the ECG, I personally asked the patient many times if he had chest discomfort; his only symptom was left hand paresthesia.
Patients can be persuaded to say that they had chest pain. Here is a scenario that I have seen many times (made a bit humorous):
Doctor:
"Are you sure you didn't have any chest pain?"
"Are you positive?!?"
"You must have had chest pain, no?"
"When did your chest pain stop?"
Patient: "OK, doctor, I did have a little chest pain, I think. Maybe a little"
Doctor: "Aha. You did have chest pain!"
And then it is easy to imagine this doctor who interviewed the patient after seeing the ECG thinks, "Those ER docs, they just can't take a good history!"
But, seriously, in order to appreciate that many patients with MI and STEMI do not have chest pain or SOB, one has to experience these patients PRIOR to the ECG. Or one must be blinded to the ECG. This is how we in the emergency department, or medics on the ambulance, experience patients: we get to know their symptoms in a blinded way, in this case before we see an ECG.
To his credit, he relented when he saw the ECG.
Door to EKG time: the door to EKG time was 3 hours in this case. But it is a miracle that any ECG was recorded. Management of this case was exemplary because any ECG was recorded. However, because it was recorded, it was recorded late, and thus the door to balloon time was long. This sort of management could harm your statistics even though it helps your patient. Institutions where a patient like this would not get an ECG would protect their DBT averages!!
STEMI patients without chest pain: In spite of a clear absence of chest pain or SOB on history done prior to the ECG, there were many mentions on the inpatient chart of the patient having had "chest discomfort" and "shortness of breath". It is very common for physicians to impute chest discomfort after seeing a STEMI on the ECG. They cannot imagine that someone can have a STEMI without any chest discomfort, or at least SOB. But this does happen. See this case in which, after seeing the ECG, I personally asked the patient many times if he had chest discomfort; his only symptom was left hand paresthesia.
Patients can be persuaded to say that they had chest pain. Here is a scenario that I have seen many times (made a bit humorous):
Doctor:
"Are you sure you didn't have any chest pain?"
"Are you positive?!?"
"You must have had chest pain, no?"
"When did your chest pain stop?"
Patient: "OK, doctor, I did have a little chest pain, I think. Maybe a little"
Doctor: "Aha. You did have chest pain!"
And then it is easy to imagine this doctor who interviewed the patient after seeing the ECG thinks, "Those ER docs, they just can't take a good history!"
But, seriously, in order to appreciate that many patients with MI and STEMI do not have chest pain or SOB, one has to experience these patients PRIOR to the ECG. Or one must be blinded to the ECG. This is how we in the emergency department, or medics on the ambulance, experience patients: we get to know their symptoms in a blinded way, in this case before we see an ECG.
Great case study - thank you!
ReplyDeleteThanks, Heidi!
DeleteGreat case. I was wondering--for a
ReplyDeleteSTEMI, it should be ECG changes and symptoms... So if he had such nonspecific symptoms, is it still considered a miss?
The universal definition of MI has many other criteria for diagnosing MI. One need not have symptoms if there is imaging or ECG evidence, in addition to at least one troponin above the 99% reference value, with a rise and/or fall. Even so, there were symptoms. They just weren't the symptoms we usually think of with coronary ischemia. Even if there were not symptoms, if the troponin was negative, and there was no wall motion abnormality: then the definition would be meaningless. The patient had coronary thrombosis, potentially deadly: definitions are almost exclusively useful for research purposes, NOT to deny therapy to patients who have pathology.
DeleteSteve Smith
Steve Smith
neat!
ReplyDeletethanks for mentioning the medics!