
Friday, November 30, 2012
Monday, November 26, 2012
Full Text of Left Bundle Branch Block Article Now Free Online
Smith SW et al. Diagnosis of ST-Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block With the ST-Elevation to S-Wave Ratio in a Modified Sgarbossa Rule
There is one rather glaring, but inconsequential, error in the article. I'm interested to see if you pick up on it, so I won't say what it is yet.
And, of course, we will publish an erratum later, unless there is a letter to the editor to which we will respond.
Don't forget: Dr. Smith's ECG Blog will be live online at 1:30 PM Central Time on Thursday, Nov. 29, 2012. Video will be broadcast directly on the blog site, and you may call in to ask a question using Skype. The Skype ID is: smithecg
There is one rather glaring, but inconsequential, error in the article. I'm interested to see if you pick up on it, so I won't say what it is yet.
And, of course, we will publish an erratum later, unless there is a letter to the editor to which we will respond.
Don't forget: Dr. Smith's ECG Blog will be live online at 1:30 PM Central Time on Thursday, Nov. 29, 2012. Video will be broadcast directly on the blog site, and you may call in to ask a question using Skype. The Skype ID is: smithecg
Wednesday, November 21, 2012
An Emergency Physician Texted Me This ECG, Asking for Help in Interpretation and for Advice in Management
I was in a meeting and received a text message: "can you look at an ECG?"
I texted back to take a photo and send it.
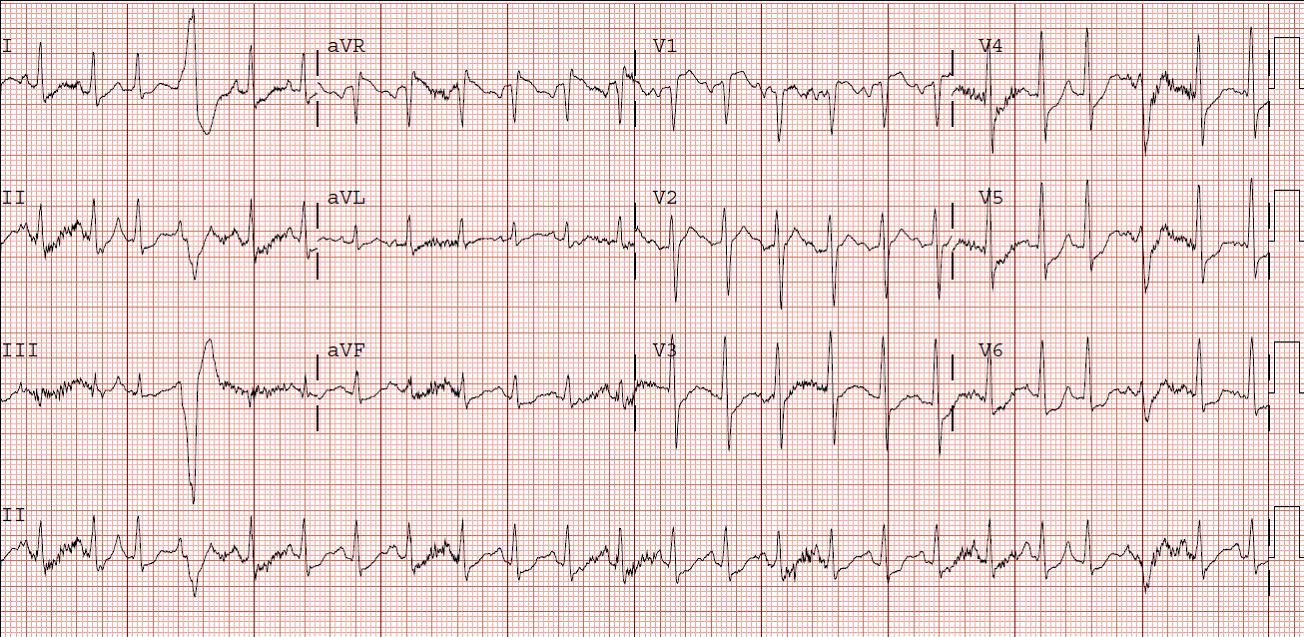
The patient is a male over 40 years of age with central chest discomfort for several hours. Here is the ECG, as texted:
Answer
I called her back and this is what I said:
I texted back to take a photo and send it.
The patient is a male over 40 years of age with central chest discomfort for several hours. Here is the ECG, as texted:
 |
| What is your diagnosis? |
Answer
I called her back and this is what I said:
“This
is a definite posterolateral MI, with an occluded artery, probably an OM, but
it is not technically a STEMI because there is not 1 mm in 2 consecutive
leads. He needs to go to the cath lab ASAP.”
How did I know this?
Because there is BOTH: minimal STE in I and aVL with
reciprocal ST depression in III, AND ST depression in V2 and V3.
Combine this with sudden onset of substernal chest pain and
you have a certain posterolateral MI.
She called the cardiologist on call and emphasized the need to go ASAP to the cath lab. The patient's pain resolved completely with intensive medical therapy, and so the urgency was less. Within a very short time, the patient underwent an angiogram that showed a 99% OM-1 occlusion and and 85% RCA. Both appeared "hazy"; both appeared to be culprits and both underwent stenting.
A subsequent echo was normal, without wall motion abnormality. Remember this!
The troponin I peaked at 58 ng/ml, so this was not a small MI.
Learning points:
- 25-30% of "NonSTEMIs" have an occluded infarct-related artery at 24 hours after presentation. (1, 2, 3)
- Many more are occluded at the time of presentation.
- This ECG would be read as "non-diagnostic" by the vast majority of interpreters. There are many "nondiagnostic" ECGs that really are diagnostic if scrutinized closely.
- Cardiac ultrasound done after resolution of ischemia is only moderately sensitive for MI.
References
1. Wang T, Zhang M, Fu
Y, et al. Incidence, distribution, and prognostic impact of occluded culprit
arteries among patients with non–ST-elevation acute coronary syndromes undergoing
diagnostic angiography Am Heart J 2009;157(4):716-23.
2. From AM, Best PJM, Lennon RJ, Rihal CS,
Prasad A. Acute Myocardial Infarction Due to Left Circumflex Artery Occlusion
and Significance of ST-Segment Elevation. Amercan Journal of Cardiology 2010;106(8):1081-5.
3. Pride YB, et al. Angiographic and clinical outcomes among patients with ACS presenting with isolated ST-Segmment Depression: A TRITON-TIMI 38 Substudy. Journal of the American College of Cardiology: Cardiovascular Interventions 2010;3(8):806-11.
Friday, November 16, 2012
Chest Pain and Right Bundle Branch Block. What is the Diagnosis?
A male in his 70's with no h/o MI or CAD presented with new onset chest pain. Here is his ED ECG:
Normally, RBBB has ST depression in right precordial leads, especially
V2 and V3 (see ECG below). Sometimes it is isoelectric. But if there is any ST segment
elevation, as in this case, it is STEMI (or RBBB with old MI and persistent ST elevation) until proven otherwise.
The emergency physician was very worried about STEMI, called the cardiologist on call, and they performed an immediate bedside echo which confirmed absence of anterior wall motion. Immediate angiogram was done and confirmed LAD occlusion, which was opened and stented.
Here is another example.
Here is a 3rd example.
Here is a 4th example.
 |
| There is sinus rhythm and right bundle branch block, and ST elevation in V1-V3. |
 |
| Baseline RBBB (normal RBBB, no STEMI). Note that there is a large R' wave in V1-V3 and discordant (opposite direction of QRS) ST segments. (Thanks to K. Wang's EKG Atlas for this image) |
The emergency physician was very worried about STEMI, called the cardiologist on call, and they performed an immediate bedside echo which confirmed absence of anterior wall motion. Immediate angiogram was done and confirmed LAD occlusion, which was opened and stented.
Here is another example.
Here is a 3rd example.
Here is a 4th example.
{kind=link}
Friday, November 9, 2012
Wide Complex Tachycardia. What is the Diagnosis?
A man in his 40's with a h/o coronary disease complained of sudden dizziness and chest pain. Medics found him with a high pulse, and rhythm strip and prehospital 12-lead (not shown) had a wide complex at a consistent rate of 135.
On arrival, here is his initial ED ECG, and is identical to the prehospital ECG and at the same rate:
So this is most likely SVT (PSVT) with aberrancy (RBBB) because: a) the typical RBBB pattern makes VT unlikely b) the absence of p-waves and the constancy of the rhythm makes sinus tach unlikely and c) flutter should have something that could be construed as flutter waves in leads II and/or V1.
Alternatively, it could be posterior fascicular ventricular tachycardia.
Therefore, adenosine was given: the patient responded with several seconds of asystole. No underlying flutter waves were uncovered and no p-waves either. The rhythm gradually returned to its baseline at a rate of 135. So it is not VT, but it was still puzzling. Either the PSVT was broken and restarted, or there is sinus tachycardia.
Having remembered Christopher Watford's post on EMCrit about the Lewis lead, I Googled "Christopher Watford" and found the post.
Just as it describes, I then:
By changing the lead orientation, one can detect atrial activity with much higher sensitivity. Our electrophysiologist learned of this age-old technique (first described by Sir Thomas Lewis in 1931) technique from his mentor, and also uses it in wide complex tachycardia to detect atrioventricular dissociation (when you see AV dissociation in wide complex tachycardia, it is diagnostic of ventricular tachycardia).
The link to Christopher's interview provides all the resources you need to learn more about the Lewis Lead.
Some Final Comments:
I have added this because of some comments/questions of whether I might treat with verapamil because this looks like verapamil sensitive idiopathic VT:
While this does look like verapamil sensitive idiopathic VT, it does have a typical bifascicular block pattern. The only thing atypical about it is the T-waves in V2 and V3, but the QRS pattern is typical for RBBB + LAFB.
The patient's baseline ECG looks exactly the same, except that it is slower (93) and the p-waves are obvious. The Lewis leads proved that it was indeed sinus tach. And with time and fluids and anxiolytics, the rate did trend down.
Sinus tach is usually compensatory to some underlying illness. Maybe the patient has dehydration, sepsis, hemorrhage, or PE. If you were to give verapamil to someone with sinus tach secondary to underlying pathology, you would harm them and perhaps provoke hypotension and shock.
Thus, I would be very careful about giving verapamil to someone with such an ECG until you have proven that it is not sinus tach.
In fact, this is what we did. My resident wanted to treat the presumed SVT with verapamil because it had apparently recurred after adenosine. I expressed my concerns as above, and that is when we did the Lewis leads.
Outcome:
The etiology of the patient's sinus tachycardia was not discovered. He later returned to the hospital for recurrent bouts of idiopathic sinus tach.
Here is his ECG 24 hours later, at a rate of 118:
Here is an ECG from 2 weeks later:
Learning Point:
When SVT with aberrancy or VT are suspected, both may be ruled out by diagnosis of sinus tachycardia using Lewis Leads. These are simple and fast.
On arrival, here is his initial ED ECG, and is identical to the prehospital ECG and at the same rate:
 |
| There is a regular, wide complex. No p-waves are seeen. The wide complex has a right bundle branch and left anterior fascicular block morphology. No flutter waves are apparent. |
Alternatively, it could be posterior fascicular ventricular tachycardia.
Therefore, adenosine was given: the patient responded with several seconds of asystole. No underlying flutter waves were uncovered and no p-waves either. The rhythm gradually returned to its baseline at a rate of 135. So it is not VT, but it was still puzzling. Either the PSVT was broken and restarted, or there is sinus tachycardia.
Having remembered Christopher Watford's post on EMCrit about the Lewis lead, I Googled "Christopher Watford" and found the post.
Just as it describes, I then:
- Placed the Right Arm electrode on the patient’s manubrium.
- Placed the Left Arm electrode on the 5th intercostal space, right sternal border.
- Placed the Left Leg electrode on the right lower costal margin.
- Monitored Lead I.
| Now p-waves are obvious (and large!) |
The link to Christopher's interview provides all the resources you need to learn more about the Lewis Lead.
Some Final Comments:
I have added this because of some comments/questions of whether I might treat with verapamil because this looks like verapamil sensitive idiopathic VT:
While this does look like verapamil sensitive idiopathic VT, it does have a typical bifascicular block pattern. The only thing atypical about it is the T-waves in V2 and V3, but the QRS pattern is typical for RBBB + LAFB.
The patient's baseline ECG looks exactly the same, except that it is slower (93) and the p-waves are obvious. The Lewis leads proved that it was indeed sinus tach. And with time and fluids and anxiolytics, the rate did trend down.
Sinus tach is usually compensatory to some underlying illness. Maybe the patient has dehydration, sepsis, hemorrhage, or PE. If you were to give verapamil to someone with sinus tach secondary to underlying pathology, you would harm them and perhaps provoke hypotension and shock.
Thus, I would be very careful about giving verapamil to someone with such an ECG until you have proven that it is not sinus tach.
In fact, this is what we did. My resident wanted to treat the presumed SVT with verapamil because it had apparently recurred after adenosine. I expressed my concerns as above, and that is when we did the Lewis leads.
Outcome:
The etiology of the patient's sinus tachycardia was not discovered. He later returned to the hospital for recurrent bouts of idiopathic sinus tach.
Here is his ECG 24 hours later, at a rate of 118:
 |
| P-waves at this slower rate are now clearly visible. The QRS morphology is identical, confirming that this rhythm had to be supraventricular. The supraventricular rhythm was sinus |
Here is an ECG from 2 weeks later:
 |
| Again, this is clearly sinus rhythm with RBBB and LAFB. |
Learning Point:
When SVT with aberrancy or VT are suspected, both may be ruled out by diagnosis of sinus tachycardia using Lewis Leads. These are simple and fast.
Saturday, November 3, 2012
ST depression, pulmonary edema, and severe hypertension: is this demand ischemia or acute coronary syndrome?
This middle-aged patient has a history of CVA and hypertension. He presented with a two hour onset of pulmonary edema and chest pressure, severely elevated blood pressure, and very tachycardic. His prehospital BP was 280/150, and it was 230/150 in the ED. He had not been taking his antihypertensives He was speaking in 1-2 word sentences and had diffuse rales. Chest xray confirmed pulmonary edema. Here is his initial ECG:
 |
| This shows horizontal ST depression in V3-V6, with STE in aVR, diagnostic of ischemia. There is no LVH. The ST depression is not secondary to LVH, but due to ischemia. As we have discussed often, the diffuse ST depression and ST elevation in lead aVR are signs of severe ischemia, usually left main stenosis or 3-vessel disease, and often occurs in patients who will need CABG. |
There are two primary possibilities:
First, the patient has hypertension which worsened, increasing afterload, leading to some pulmonary edema and demand ischemia and worsening in a vicious cycle.
Second, he had an acute coronary syndrome which initiated the increase in end diastolic pressure, leading to pulmonary edema, increased catecholamine output, increased BP and HR, with a different kind of vicious cycle.
The first possibility is made significantly less likely by the absence of LVH. Patients with this syndrome of demand ischemia almost always have LVH on the ECG. If this was all initiated by hypertension, then managing the demand by treating the blood pressure and other physiologic variables such as pulmonary edema, hypoxia, etc. would result in resolution of the ischemia, and could be measured by resolving ST depression on the ECG.
Either way, it is necessary to manage the airway, ventilation and oxygenation, treat the hypertension (high dose intravenous nitrates are a fine method), and normalize other important physiologic variables such as anemia and electrolytes.
However, in the second case, aggressive antiplatelet and antithrombotic therapy is essential. If there is no resolution of ischemia with these aggressive medical measures, then urgent cardiac catheterization is indicated and an interventionalist should be consulted immediately.
In this case, the physiologic derangements were well managed and the patient stabilized with noninvasive positive pressure ventilation without endotracheal intubation. The BP came down with 160 mcg/min of IV nitroglycerine, and 1.25 mg of IV enalapril.
At this point, it is essential to obtain a followup ECG to confirm resolution of ischemia. However, in this case, no followup ECG was obtained before admission because the clinicians assumed that the ischemia was all due to demand from hypertension.
Very soon after admission, the patient's chest pain increased and the following ECG was recorded 2 hours after the first ECG:
 |
| This ECG shows new Right Bundle Branch Block and Left Anterior Fascicular block, with marked ischemic ST elevation in leads V1-V5, I, and aVL, diagnostic of a proximal LAD occlusion. The bifascicular block is a sign of severe ischemia and is frequently seen in severe left main ACS. |
Learning points:
1) Flash pulmonary edema may be from demand ischemia, especially with hypertension, but it may be due to severe acute coronary syndrome.
2) When due to hypertension, there is almost always LVH on the ECG
3) Ischemic ST depression is associated with very high risk.
4) If ischemic ST depression is refractory to management of hemodynamic variables, hemoglobin, oxygenation (i.e., refractory to management of those variables that contribute to demand ischemia), aggressive medical treatment for ACS must be started.
5) If the ischemia is refractory to maximal medical management, angiogram with possible PCI is indicated.
6) Always repeat the ECG to assess management of ischemia.
7) In ACS, thrombus may be partially occlusive and result in ST depression. It may be fully occlusive, without collaterals, resulting in ST elevation. Or it may start as partly occlusive and extend to complete occlusion, as in this case.
8) New Right Bundle Branch block in the presence of STEMI has a very high mortality.
11/7/09