
Benign T-wave Inversion from HQMedEd on Vimeo.
There are many etiologies of T-wave inversion. We are most worried about ischemic T-wave inversion. Wellens' syndrome is particularly dangerous, as it signifies an unstable critical LAD stenosis. I have several posts on this; here is one that shows the entire evolution.
Another etiology is "Benign T-wave Inversion", which has long been recognized. I first saw it described in Chou's textbook. It is a normal variant associated with early repolarization. K. Wang recently studied it. He reviewed ECGs from all 11,424 patients who had at least one recorded during 2007 at Hennepin County Medical Center (where I work) and set aside the 101 cases of benign T-wave inversion. 97 were black. 3.7% of black men and 1% of black women had this finding. 1 of 5099 white patients had it. Aside from an 8.8% incidence (9 of 109) black males aged 17-19, it was evenly distributed by age group.
I have reviewed these 101 ECGs, and what strikes me is:
1. There is a relatively short QT interval (QTc < 425ms)
2. The leads with T-wave inversion often have very distinct J-waves.
3. The T-wave inversion is usually in leads V3-V6 (in contrast to Wellens' syndrome, in which they are V2-V4)
4. The T-wave inversion does not evolve and is generally stable over time (in contrast to Wellens', which evolves).
5. The leads with T-wave inversion (left precordial) usually have some ST elevation
6. Right precordial leads often have ST elevation typical of classic early repolarization
7. The T-wave inversion in leads V4-V6 is preceded by minimal S-waves
8. The T-wave inversion in leads V4-V6 is preceded by high R-wave amplitude
9. II, III, and aVF also frequently have T-wave inversion.
Below are 5 examples, followed by a case of Wellens.'
I show you the LAD-BER formula calculations, but remember, strictly speaking, this was not studied in ECGs with: 1) T-wave inversion, 2) coved (upwardly convex) ST segments, or 3) LVH.
Here is the formula; there is an excel spreadsheet down the right side of this blog: (1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) - (0.326 x R-wave Amplitude in V4 in mm). A value greater than 23.4 is quite sensitive and specific for LAD occlusion.
 |
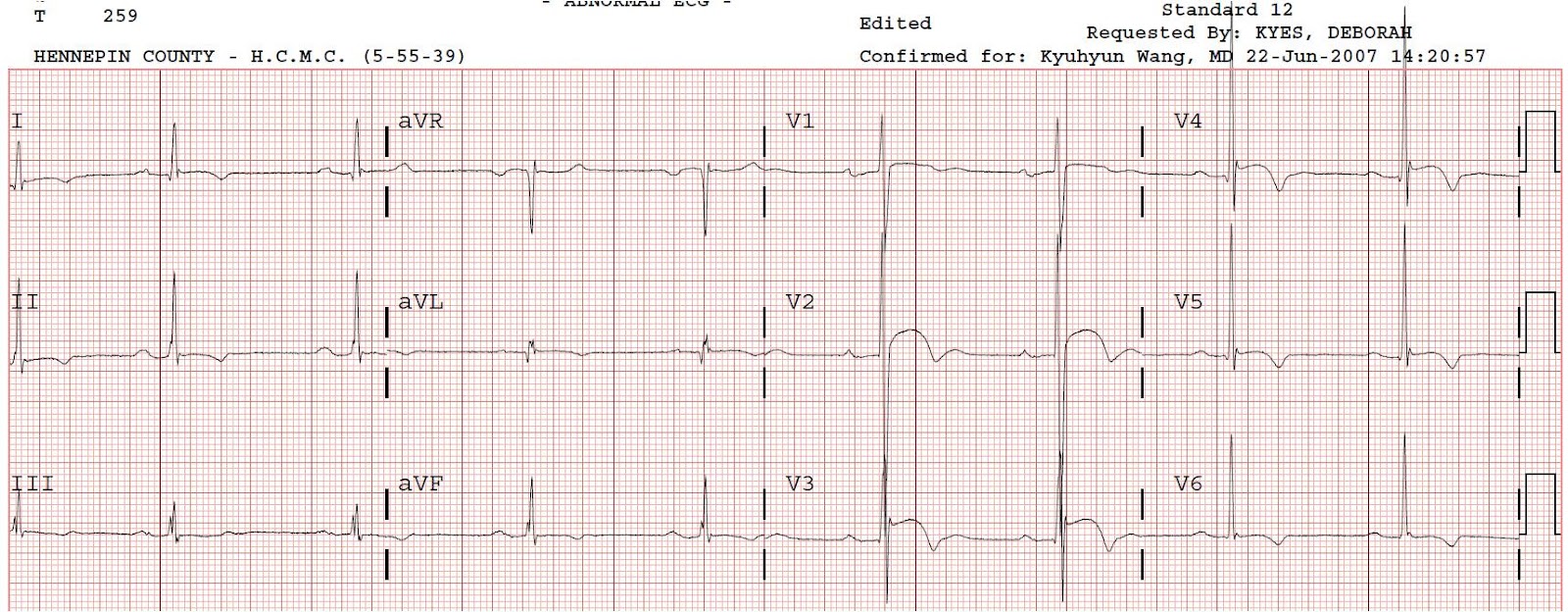
| Benign T-wave inversion: There is ST elevation in V2 and V3, with T-wave inversion in left precordial leads. QTc = 395ms, formula value (to determine if the STE is STEMI or not) = 21.13 (< 23.4 is early repol). Note the prominent J-waves, the minimal S-waves and the prominent R amplitude in leads with T-wave inversion. |
 |
| Benign T-wave Inversion: This has some scary looking STE and TWI. QTc is 415ms and formula value is 21.39. |
 |
| Benign t-wave inversion. QTc = 415, formula = 18.5 |
 |
| Benign T-wave inversion and probable LVH. Scary ST elevation, right? But QTc is 421ms and formula value is 20.17. |
 |
| Benign T-wave Inversion? QTc 398, formula 17.6. This one was not stable. The next day it was gone. It was recorded in a young black male with chest pain. There were negative serial troponins but no angiogram. Dr. Wang considered it to be BTWI. |
 |
| Wellens' syndrome. Note the evolution from A to C. It begins with terminal T-wave inversion (biphasic) in lead V2, later extends to V3 and V4, and still later becomes deep and symmetric and only then extends to V6. There was a critical LAD stenosis. In this case I do not know what the computerized QTc was. This is taken from an article I wrote in EM Clinics of North America 2006;24(1):53-89. |
Dr. Smith,
ReplyDeletein the 5 examples of BTWI on your video, every one of them had small T wave inversions in leads II, and aVF...3 out of 5 had T wave inversions in I and III as well.
Is there any significance to the diagnosis of BTWI and the T wave inversions in the limb leads?
thanks,
DavidB
Dave,
ReplyDeleteGood point!
I've been so focused on the precordial leads, I didn't even noticed that.
Steve Smith
Sir,
ReplyDeleteFrom the strips you showed, the aVL's had that S that we see in repolarization abnormalities. Is there a value for its sn/sp of being benign or not benign.
I'm not sure what you're referring to ????
ReplyDeleteSorry for that description but what I mean is the terminal nib or what seems to be a distortion at the end of the QRS complex in aVL's (strips 1-5 in the BTWI images) or can we say r. They seem to have same morphology on the chest leads showing repolarization abnormalities. Does it have any significance (like sn/sp) (in this scenario) or they are just present on these sample strips?
ReplyDeleteI hadn't noticed and I'm not sure. But good observation!
ReplyDeleteHello Dr Smith, I wanted to discuss a case with yourself. I was asked to give advice recently for a young 37 year old, male, south east asian patient. He was admitted with headache, no chest pain. Had a recent fall, subsequently developed headache. CT head was fine. He had t wave inversions in I,avl, v5 and v6 with biphasic t wave in v1 and v2 as in wellen syndrome. Although he did not have any chest pain but he had risk factors as increased cholesterol, +ve family history and he was a smoker. i know we do not treat ECG and we treat the patient but I was kind of reluctant to discharge him with that kind of Ecg and with risk factors. What would your advice be?
ReplyDeleteIf you're worried, have him do a stress test. Feel free to send the ECG to: dr.smiths.ecg.blog@gmail.com
DeleteHey Dr. Smith , u did great job in educating us in ECGs and the cases thank u Sir
DeleteI had question , difference betwern Accelerated Idioventricular rythm and Interventricular conduction defect , and are both benign and needs no ttt?
Also wanted to ask , can T wave inversions be a sign of new ischemia without ST depression? And should one worry if it is in single lead? I read that T wave inversion can be normal variant in lll and avf and avl
Last question and am sorry , what if one with BER or BTWI presented with Acute coronary syndrome , what his ECG will look like then ? Like his BER and BTWI can lead me astray if he develops Acute MI right? Sorry for asking too much
What the the stress test gonna reveal if thats pathological biphasic T wave? Like shall i see ST elevation for example or what ? Thank u Dr Smith
DeleteWhat if I have T wave inversions in V3 and V4? Is it normal? If not what is it due to?
ReplyDeleteThat is variable and I would need to see the ECG you are referring to. You should watch this lecture on T-wave inversion: http://hqmeded-ecg.blogspot.com/2015/05/new-40-minute-lecture-on-t-wave.html
DeleteI have seen the video but couldn't determine what's wrong in my ECG
DeleteWhat if I have T wave inversion in V3 and V4? Is it normal? If not what could have caused it to be so?
ReplyDeletesend it to: dr.smiths.ecg.blog@gmail.com
ReplyDeleteDr Smith, how to distinguish benign T wave inversion from T wave inversion due to apical hypertrophic cardiomyopathy? I find them very similar.
ReplyDeleteSir t inversion in 111 and avf. Is it normal
ReplyDeleteIt is a normal finding in BTWI
DeleteDr Smith, t wave inversion in leads III, avf and v1 is abnormal or a variable?
ReplyDeleteIt may be present with benign T-wave inversion.
DeleteThese are applicable for 18-19 years black men or is it the same for 33 years male as well?
ReplyDeleteSame
DeleteHello Dr.Smith,
ReplyDeleteWhat about biphasic T wave inversion in lead ii, iii and avf, and symmetric t wave inversion in precordial leads V3-v6?
As you can see, these examples have all of the above.
DeleteSo it means biphasic t waves in limb leads (lead ii,iii and avf) are benign?
ReplyDeleteAnd one more question Dr.Smith, i have these changes whenever I take ECG, you told it will not evolve , does that mean these chenges remain forever in the ecg?
That it will not evolve means over hours to days, as Wellens waves will always evolve. Over months to years evolution is likely.
DeleteThank you doctor Smith. As you said these all are benign changes, and do you suspect these changes will remain permanent for ages? or will there be any progressive changes after few years?
ReplyDeleteI think they go away with time, but I do not have proof of this.
DeleteSteve smith sir hi, t wave inversion in just one lead 3 is it benighn.
ReplyDeleteHi. In my opinion — it is IMPOSSIBLE to answer the question of whether "T wave inversion in just 1 lead = lead 3 is benign or not" UNLESS you: i) Know the context in which this T wave inversion occurs; and ii) See the ACTUAL ECG itself — because there may be other subtle abnormalities that I might see that perhaps you did not AND/OR we need to know what the frontal plane axis is; what lead aVL looks like; whether there is incomplete or complete RBBB, etc. Feel free to send the tracing to our contact E-mail address (near the top of the righthand column) together with the clinical history — :)
DeleteCan i ask the depth of the T wave inversion says something or not specific to anything? Like can someone have deep T wave inversion and be benign not pathological? Thanks
DeleteI would say, without hard data, that if it is very deep it is due to LVH, HOCM, or ischemia. But what is the definition of very deep? Look at these examples.
Delete